

Deviation analysis of C2 translaminar screw placement assisted by a novel rapid prototyping drill template: a cadaveric study
- PMID: 24005997
- PMCID: PMC3843787
- DOI: 10.1007/s00586-013-2993-0
Deviation analysis of C2 translaminar screw placement assisted by a novel rapid prototyping drill template: a cadaveric study
Abstract
Purpose: The goal of this study is to evaluate the accuracy of patient-specific CT-based rapid prototype drill templates for C2 translaminar screw insertion.
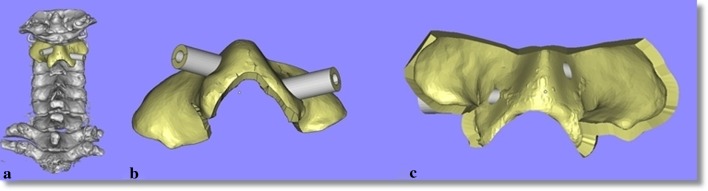
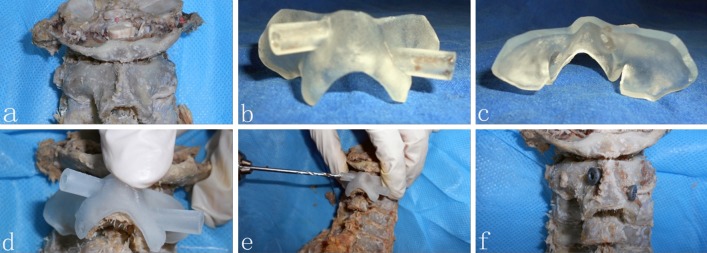
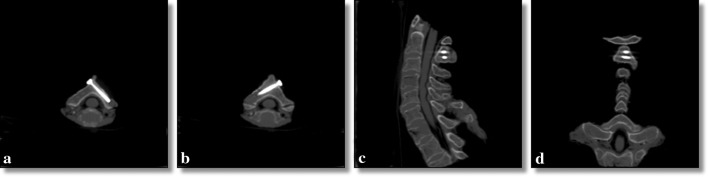
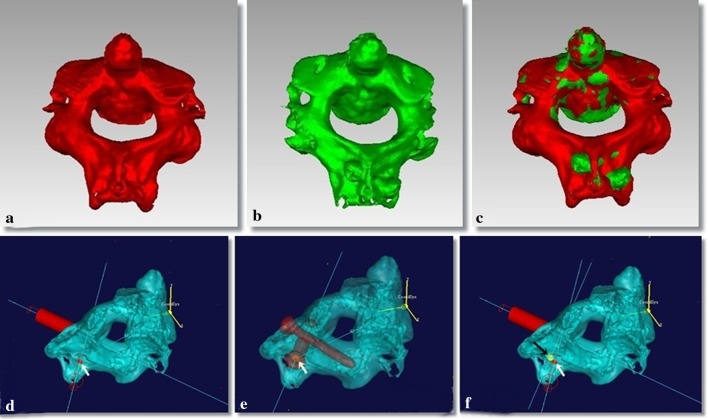
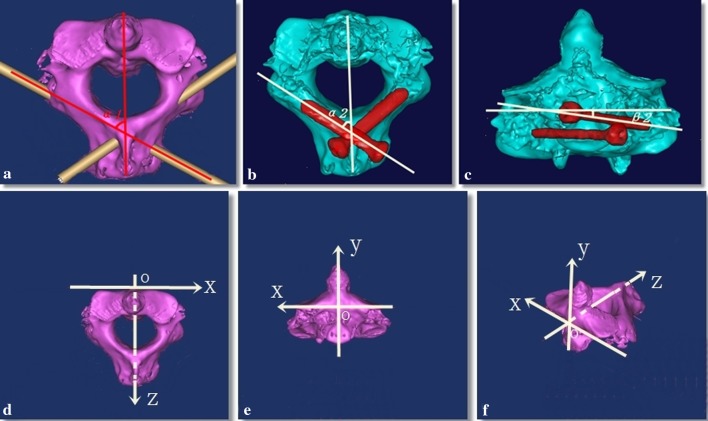
Methods: Volumetric CT scanning was performed in 32 cadaveric cervical spines. Using computer software, the authors constructed drill templates that fit onto the posterior surface of the C2 vertebrae with drill guides to match the slope of the patient's lamina. Thirty-two physical templates were created from the computer models using a rapid prototyping machine. The drill templates were used to guide drilling of the lamina and post-operative CT images were obtained. The entry point and direction of the planned and inserted screws were measured and compared.
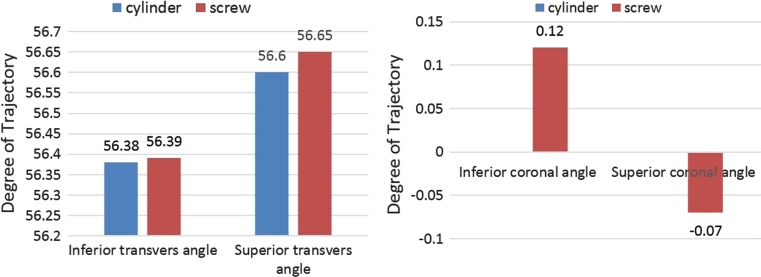
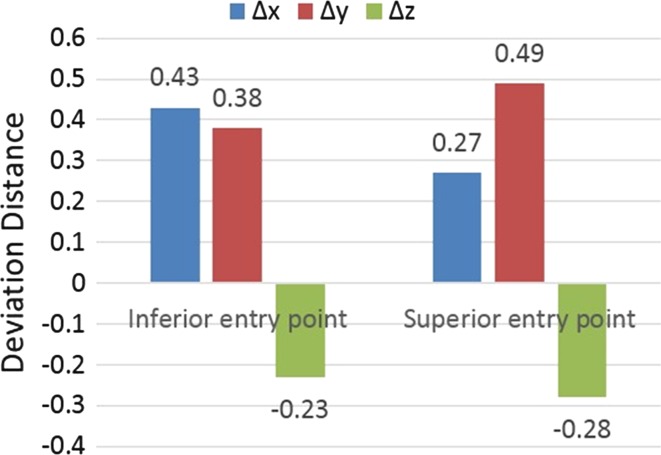
Results: Sixty-four C2 translaminar screws were placed without violating the cortical bone of a single lamina. The bilateral average transverse angle of intended and actual screw for C2TLS was 56.60 ± 2.22°, 56.38 ± 2.51°, 56.65 ± 2.24°, 56.39 ± 2.45°. The bilateral mean coronal angle of the planned and actual screw for C2TLS was 0°, 0°, -0.07 ± 0.32°, 0.12 ± 0.57°. The average displacement of the entry point of the superior and inferior C2TLS in the x, y, z axis was 0.27 ± 0.85, 0.49 ± 1.46, -0.28 ± 0.69, 0.43 ± 0.88, 0.38 ± 1.51, 0.23 ± 0.64 mm.
Conclusion: The small deviations seen are likely due to human error in the form of small variations in the surgical technique and use of software to design the prototype. This technology improves the safety profile of this fixation technique and should be further studied in clinical applications.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
