

Nonrigid autofocus motion correction for coronary MR angiography with a 3D cones trajectory
- PMID: 24006292
- PMCID: PMC3942375
- DOI: 10.1002/mrm.24924
Nonrigid autofocus motion correction for coronary MR angiography with a 3D cones trajectory
Abstract
Purpose: To implement a nonrigid autofocus motion correction technique to improve respiratory motion correction of free-breathing whole-heart coronary magnetic resonance angiography acquisitions using an image-navigated 3D cones sequence.
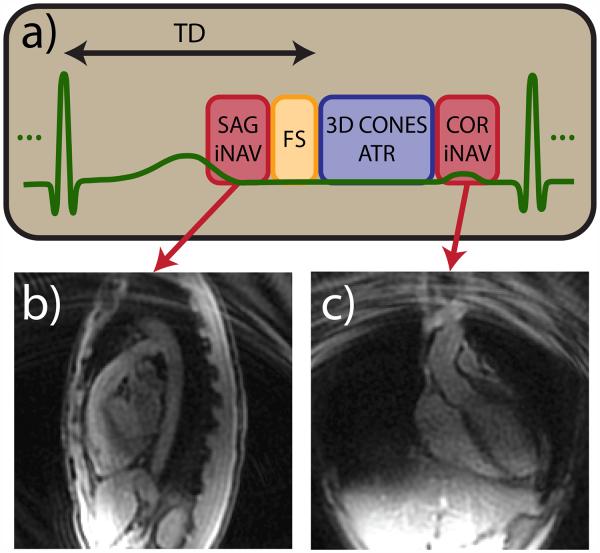
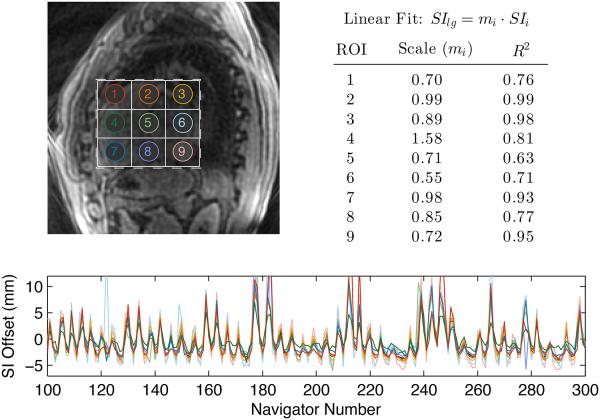
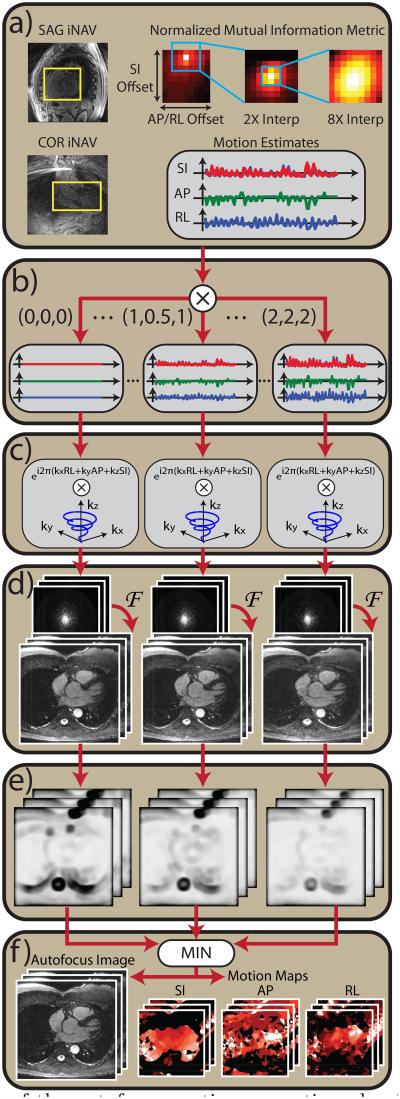
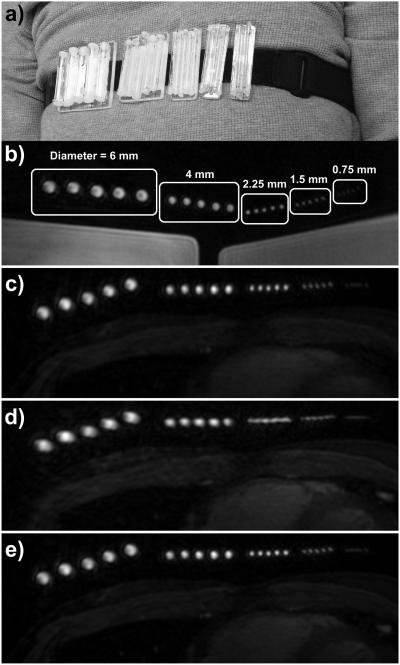
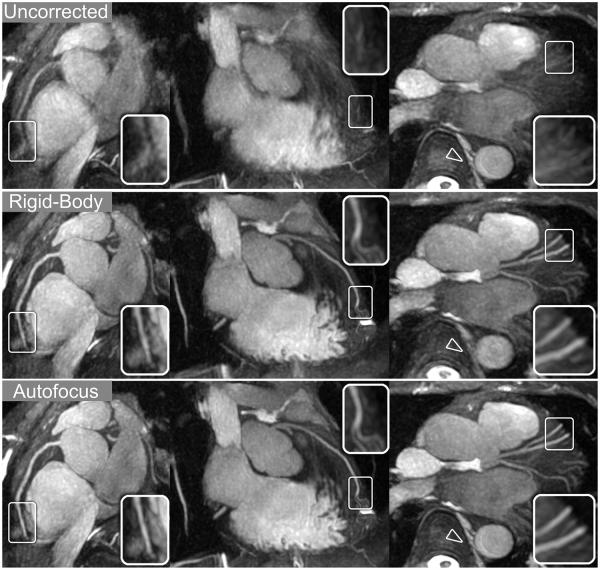
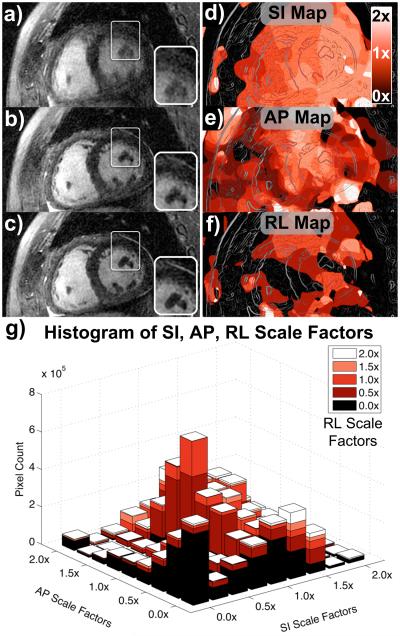
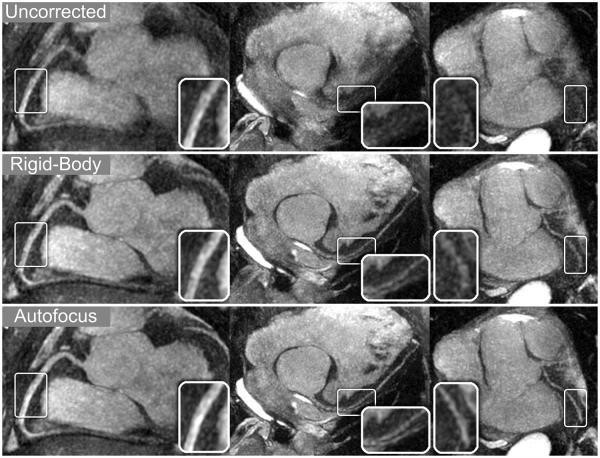
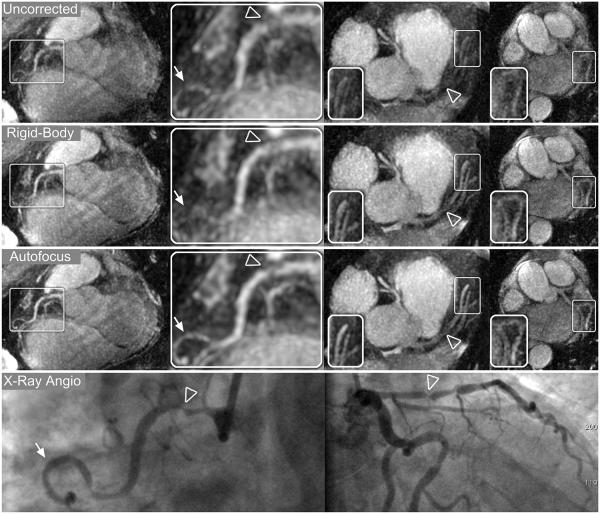
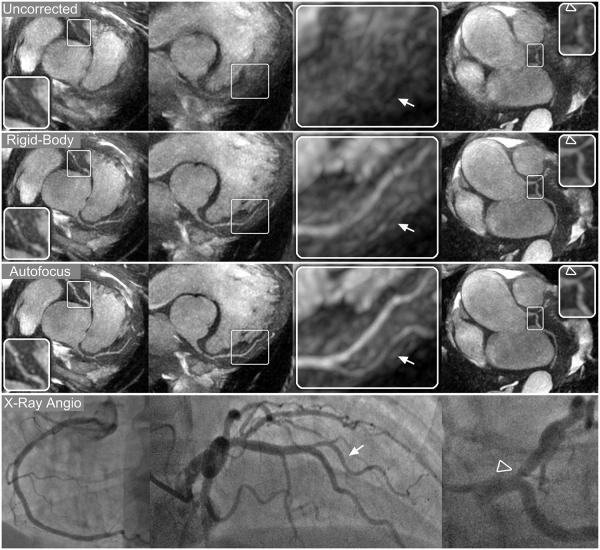
Methods: 2D image navigators acquired every heartbeat are used to measure superior-inferior, anterior-posterior, and right-left translation of the heart during a free-breathing coronary magnetic resonance angiography scan using a 3D cones readout trajectory. Various tidal respiratory motion patterns are modeled by independently scaling the three measured displacement trajectories. These scaled motion trajectories are used for 3D translational compensation of the acquired data, and a bank of motion-compensated images is reconstructed. From this bank, a gradient entropy focusing metric is used to generate a nonrigid motion-corrected image on a pixel-by-pixel basis. The performance of the autofocus motion correction technique is compared with rigid-body translational correction and no correction in phantom, volunteer, and patient studies.
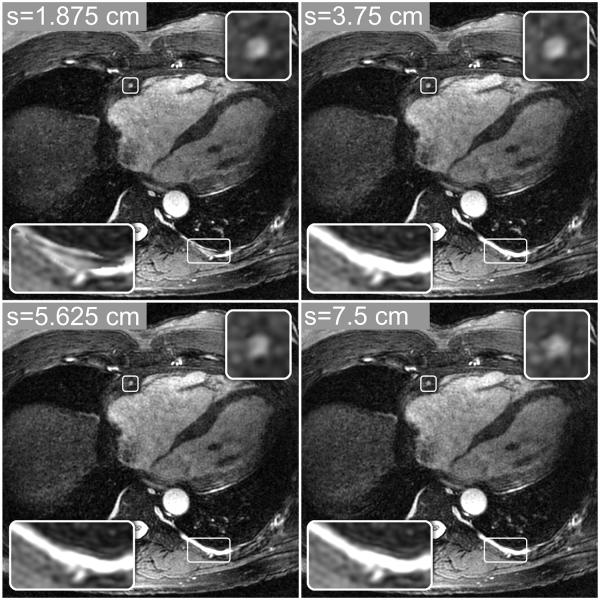
Results: Nonrigid autofocus motion correction yields improved image quality compared to rigid-body-corrected images and uncorrected images. Quantitative vessel sharpness measurements indicate superiority of the proposed technique in 14 out of 15 coronary segments from three patient and two volunteer studies.
Conclusion: The proposed technique corrects nonrigid motion artifacts in free-breathing 3D cones acquisitions, improving image quality compared to rigid-body motion correction.
Keywords: autofocus; coronary angiography; motion correction; navigator image; nonrigid.
Copyright © 2013 Wiley Periodicals, Inc.
Figures
References
-
- Scott AD, Keegan J, Firmin DN. Motion in cardiovascular MR imaging. Radiology. 2009;250:331–351. - PubMed
-
- Goldfarb JW, Edelman RR. Coronary arteries: breath-hold, gadolinium-enhanced, three-dimensional MR angiography. Radiology. 1998;206:830–834. - PubMed
-
- Li D, Carr JC, Shea SM, Zheng J, Deshpande VS, Wielopolski PA, Finn JP. Coronary arteries: magnetization-prepared contrast-enhanced three-dimensional volume-targeted breath-hold MR angiography. Radiology. 2001;219:270–277. - PubMed
-
- Niendorf T, Hardy CJ, Giaquinto RO, Gross P, Cline HE, Zhu Y, Kenwood G, Cohen S, Grant AK, Joshi S, Rofsky NM, Sodickson DK. Toward single breath-hold whole-heart coverage coronary MRA using highly accelerated parallel imaging with a 32-channel MR system. Magn Reson Med. 2006;56:167–176. - PubMed
-
- Wang Y, Rossman PJ, Grimm RC, Riederer SJ, Ehman RL. Navigator-echo-based real-time respiratory gating and triggering for reduction of respiration effects in three dimensional coronary MR angiography. Radiology. 1996;198:55–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
