

Near-infrared spectroscopy StO2 monitoring to assess the therapeutic effect of drotrecogin alfa (activated) on microcirculation in patients with severe sepsis or septic shock
- PMID: 24007807
- PMCID: PMC3847092
- DOI: 10.1186/2110-5820-3-30
Near-infrared spectroscopy StO2 monitoring to assess the therapeutic effect of drotrecogin alfa (activated) on microcirculation in patients with severe sepsis or septic shock
Abstract
Background: Sepsis is a leading cause of death despite appropriate management. There is increasing evidence that microcirculatory alterations might persist independently from macrohemodynamic improvement and are related to clinical evolution. Future efforts need to be directed towards microperfusion monitoring and treatment. This study explored the utility of thenar muscle oxygen saturation (StO2) and its changes during a transient vascular occlusion test (VOT) to measure the microcirculatory response to drotrecogin alfa (activated) (DrotAA) in septic patients.
Methods: A prospective, observational study was performed in three general intensive care units at three university hospitals. We studied 58 patients with recent onset of severe sepsis or septic shock and at least two organ dysfunctions. Thirty-two patients were treated with DrotAA and 26 were not treated because of formal contraindication. StO2 was monitored using near-infrared spectroscopy (NIRS), and VOT was performed to obtain deoxygenation (DeOx) and reoxygenation (ReOx) slopes. Measurements were obtained before DrotAA was started and were repeated daily for a 96-hour period.
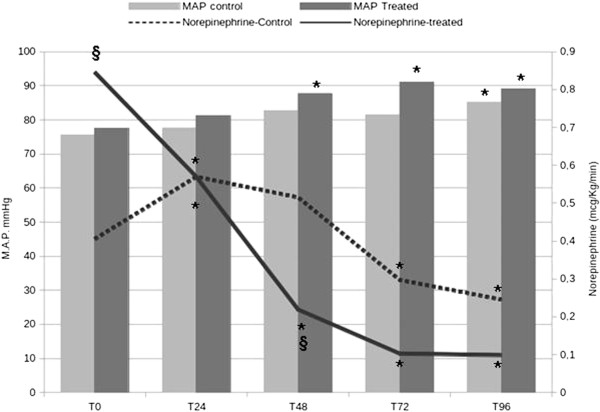
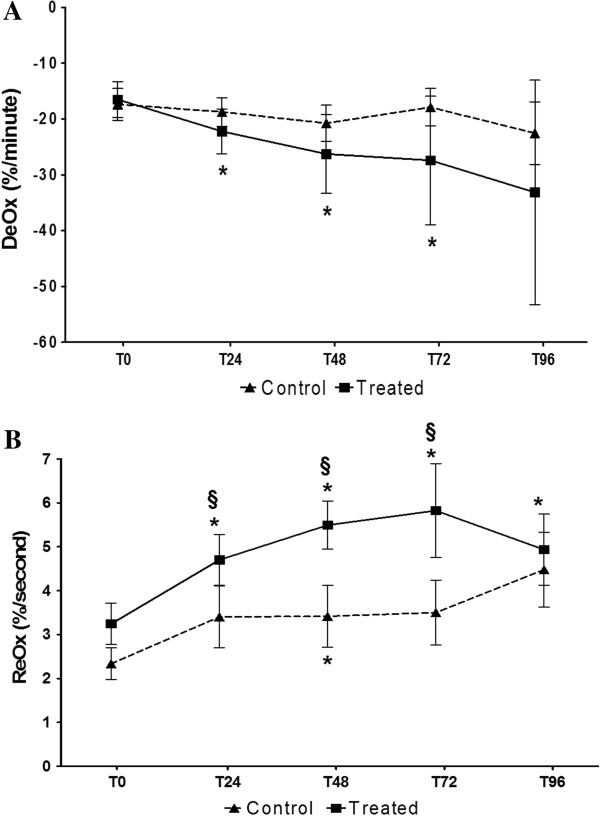
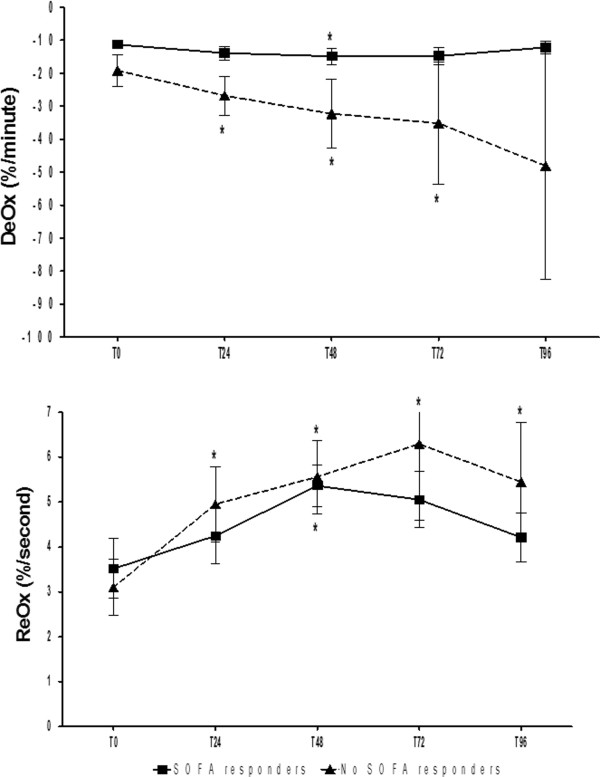
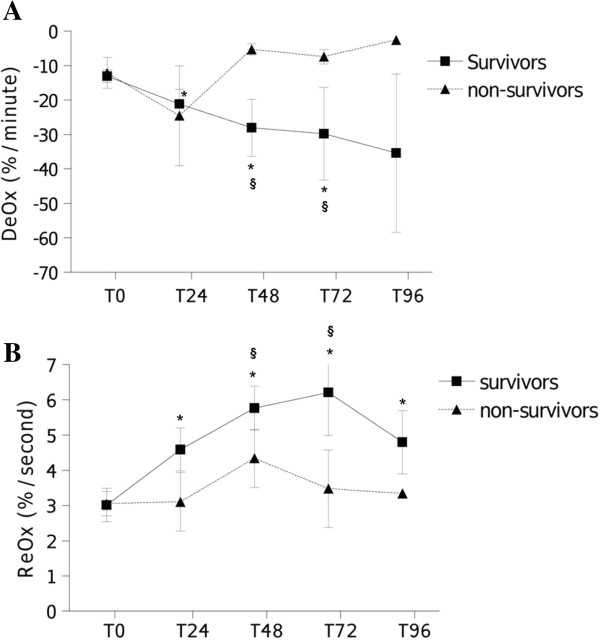
Results: Patients' characteristics, outcome, severity, and baseline values of StO2, DeOx, and ReOx did not differ between groups. Treated patients significantly improved DeOx and ReOx values over time, whereas control patients did not. In treated patients, ReOx improvements were correlated to norepinephrine dose reductions. Early clinical response (SOFA improvement after 48 hours of treatment) was not associated to changes in VOT-derived slopes. In the treated group, the relative improvement of DeOx within 48 hours was able to predict mortality (AUC 0.91, p < 0.01).
Conclusions: In patients with severe sepsis or septic shock, DrotAA infusion was associated with improvement in regional tissue oxygenation. The degree of DeOx amelioration after 2 days in treated patients predicted mortality with high sensitivity and specificity. Thus, StO2 derived variables might be useful to evaluate the microcirculatory response to treatment of septic shock.
Figures
References
-
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut J-F, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent J-L. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. 2008;3:17–60. doi: 10.1007/s00134-007-0934-2. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
