

Neural tube defects--disorders of neurulation and related embryonic processes
- PMID: 24009034
- PMCID: PMC4023228
- DOI: 10.1002/wdev.71
Neural tube defects--disorders of neurulation and related embryonic processes
Abstract
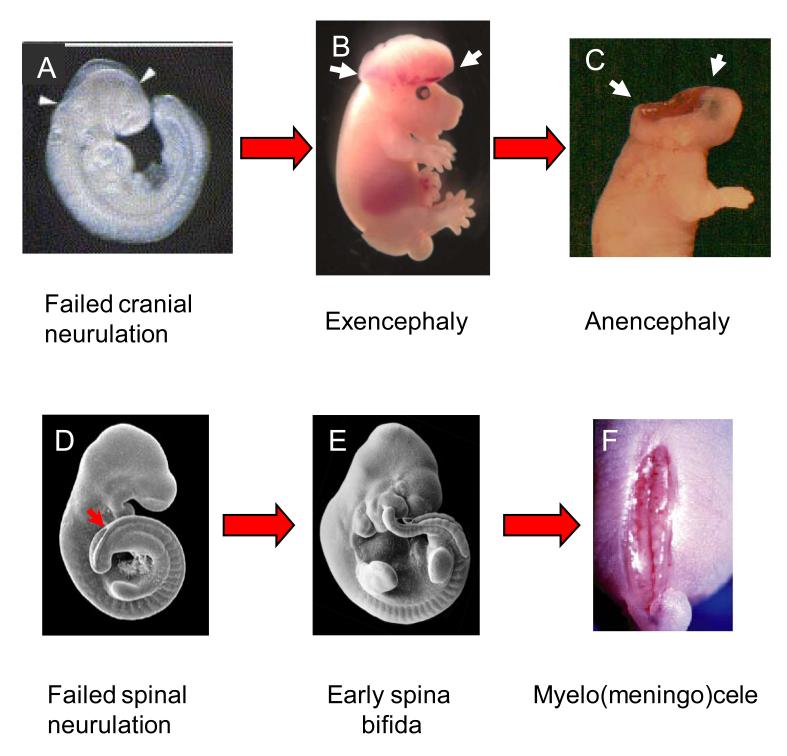
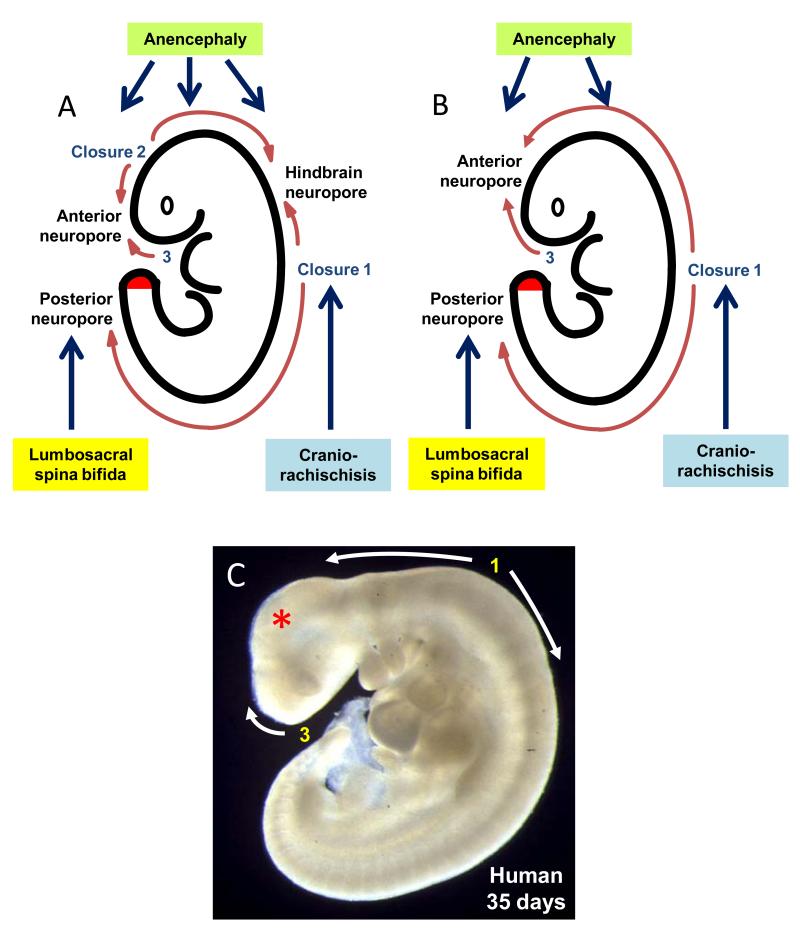
Neural tube defects (NTDs) are severe congenital malformations affecting 1 in every 1000 pregnancies. 'Open' NTDs result from failure of primary neurulation as seen in anencephaly, myelomeningocele (open spina bifida), and craniorachischisis. Degeneration of the persistently open neural tube in utero leads to loss of neurological function below the lesion level. 'Closed' NTDs are skin-covered disorders of spinal cord structure, ranging from asymptomatic spina bifida occulta to severe spinal cord tethering, and usually traceable to disruption of secondary neurulation. 'Herniation' NTDs are those in which meninges, with or without brain or spinal cord tissue, become exteriorized through a pathological opening in the skull or vertebral column (e.g., encephalocele and meningocele). NTDs have multifactorial etiology, with genes and environmental factors interacting to determine individual risk of malformation. While over 200 mutant genes cause open NTDs in mice, much less is known about the genetic causation of human NTDs. Recent evidence has implicated genes of the planar cell polarity signaling pathway in a proportion of cases. The embryonic development of NTDs is complex, with diverse cellular and molecular mechanisms operating at different levels of the body axis. Molecular regulatory events include the bone morphogenetic protein and Sonic hedgehog pathways which have been implicated in control of neural plate bending. Primary prevention of NTDs has been implemented clinically following the demonstration that folic acid (FA), when taken as a periconceptional supplement, can prevent many cases. Not all NTDs respond to FA, however, and adjunct therapies are required for prevention of this FA-resistant category.
Copyright © 2012 Wiley Periodicals, Inc.
Figures
References
-
- Dolk H, Loane M, Garne E. The prevalence of congenital anomalies in Europe. Adv Exp Med Biol. 2010;686:349–364. - PubMed
-
- Mitchell LE. Epidemiology of neural tube defects. Am J Med Genet C Semin Med Genet. 2005;135:88–94. - PubMed
-
- Wood LR, Smith MT. Generation of anencephaly: 1. Aberrant neurulation and 2. Conversion of exencephaly to anencephaly. J Neuropath exp Neurol. 1984;43:620–633. - PubMed
-
- Seller MJ. Sex, neural tube defects, and multisite closure of the human neural tube. Am J Med Genet. 1995;58:332–336. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
