

Serum phosphorus levels and pill burden are inversely associated with adherence in patients on hemodialysis
- PMID: 24009281
- PMCID: PMC4209875
- DOI: 10.1093/ndt/gft280
Serum phosphorus levels and pill burden are inversely associated with adherence in patients on hemodialysis
Abstract
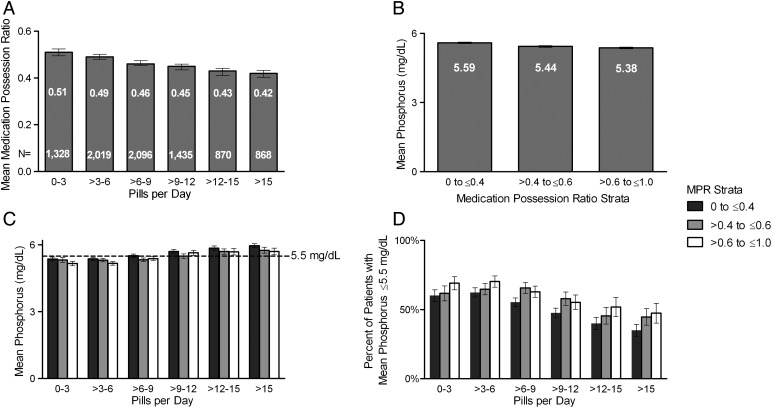
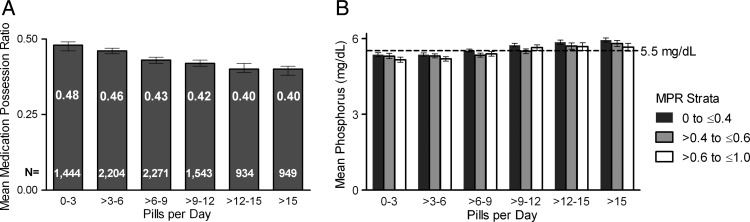
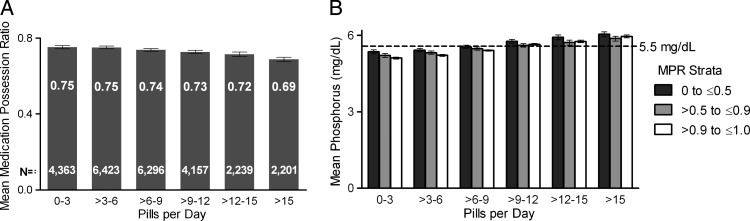
Background: Phosphate binders (PBs) account for about one half of the daily pill burden for US hemodialysis (HD) patients, which may reduce adherence. Adherence can be estimated by the medication possession ratio (MPR), which is defined as the proportion of time a patient had sufficient medication to have taken it as prescribed. Gaps of time between prescription fills lower the patient's MPR. We assessed the association of PB pill burden and adherence (MPR) with phosphorus goal attainment.
Methods: Using pharmacy management program data, HD patients on PB monotherapy were tracked from first PB fill during 1 January 2007-30 June 2011 for 1 year, or until PB change or censoring. Data were assessed with generalized linear models.
Results: We analyzed 8616 patients. Higher pill burden was associated with lower adherence. Lower adherence tended to be associated with higher mean phosphorus levels and lower percentage of patients with serum phosphorus ≤5.5 mg/dL (P < 0.001). The association between adherence and these clinical outcomes was most pronounced in the lowest and highest pill burden strata (<3, >3-6, >12-15, >15).
Conclusions: Adherence, as measured by the MPR, was negatively related to higher pill burden and phosphorus levels and positively related to patients in the phosphorus target range. Within pill burden strata, phosphorus increased and patients in the target range generally decreased with decreasing adherence, suggesting that patients prescribed fewer PB pills are less likely to have treatment gaps, and may be more likely to achieve phosphorus targets.
Keywords: adherence; hemodialysis; phosphate binders; pill burden; retrospective study.
© The Author 2013. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
Similar articles
-
Pill burden, adherence, hyperphosphatemia, and quality of life in maintenance dialysis patients.Clin J Am Soc Nephrol. 2009 Jun;4(6):1089-96. doi: 10.2215/CJN.00290109. Epub 2009 May 7. Clin J Am Soc Nephrol. 2009. PMID: 19423571 Free PMC article.
-
Phosphate binder pill burden, adherence, and serum phosphorus control among hemodialysis patients converting to sucroferric oxyhydroxide.Int J Nephrol Renovasc Dis. 2019 Jan 22;12:1-8. doi: 10.2147/IJNRD.S182747. eCollection 2019. Int J Nephrol Renovasc Dis. 2019. PMID: 30774412 Free PMC article.
-
Phosphate binder pill burden, patient-reported non-adherence, and mineral bone disorder markers: Findings from the DOPPS.Hemodial Int. 2016 Jan;20(1):38-49. doi: 10.1111/hdi.12315. Epub 2015 May 14. Hemodial Int. 2016. PMID: 25975222 Free PMC article.
-
Intensive Hemodialysis, Mineral and Bone Disorder, and Phosphate Binder Use.Am J Kidney Dis. 2016 Nov;68(5S1):S24-S32. doi: 10.1053/j.ajkd.2016.05.024. Am J Kidney Dis. 2016. PMID: 27772640 Review.
-
Sucroferric oxyhydroxide for hyperphosphatemia: a review of real-world evidence.J Nephrol. 2022 Apr;35(3):875-888. doi: 10.1007/s40620-021-01241-5. Epub 2022 Feb 9. J Nephrol. 2022. PMID: 35138627 Free PMC article. Review.
Cited by
-
Assessment of Dietary Folate Intake and Pill Burden among Saudi Patients on Maintenance Hemodialysis.Int J Environ Res Public Health. 2021 Dec 2;18(23):12710. doi: 10.3390/ijerph182312710. Int J Environ Res Public Health. 2021. PMID: 34886434 Free PMC article.
-
Effectiveness of sucroferric oxyhydroxide in patients on on-line hemodiafiltration in real-world clinical practice: A retrospective study.J Bras Nefrol. 2019 Apr-Jun;41(2):224-230. doi: 10.1590/2175-8239-JBN-2018-0142. Epub 2019 Feb 4. J Bras Nefrol. 2019. PMID: 30742699 Free PMC article.
-
Phosphate binder in dialysis: a cross-sectional study of patients' adherence and pill burden.J Bras Nefrol. 2025 Jan-Mar;47(1):e20240075. doi: 10.1590/2175-8239-JBN-2024-0075en. J Bras Nefrol. 2025. PMID: 39835716 Free PMC article.
-
A real-world analysis of the influence of age on maintenance hemodialysis patients: managing serum phosphorus with sucroferric oxyhydroxide as part of routine clinical care.Int Urol Nephrol. 2023 Feb;55(2):377-387. doi: 10.1007/s11255-022-03327-w. Epub 2022 Aug 11. Int Urol Nephrol. 2023. PMID: 35953565 Free PMC article.
-
Phosphate binders in dialysis: better satisfied than sorry.Clin Kidney J. 2021 May 19;14(8):1859-1860. doi: 10.1093/ckj/sfab093. eCollection 2021 Aug. Clin Kidney J. 2021. PMID: 34345407 Free PMC article.
References
-
- K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis. 2003;42:S1–S201. - PubMed
-
- Block GA, Hulbert-Shearon TE, Levin NW, et al. Association of serum phosphorus and calcium x phosphate product with mortality risk in chronic hemodialysis patients: a national study. Am J Kidney Dis. 1998;31:607–617. - PubMed
-
- Marchais SJ, Metivier F, Guerin AP, et al. Association of hyperphosphataemia with haemodynamic disturbances in end-stage renal disease. Nephrol Dial Transplant. 1999;14:2178–2183. - PubMed
-
- Lowrie EG, Lew NL. Death risk in hemodialysis patients: the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am J Kidney Dis. 1990;15:458–482. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
