

Sensitization from transfusion in patients awaiting primary kidney transplant
- PMID: 24009295
- PMCID: PMC3811060
- DOI: 10.1093/ndt/gft362
Sensitization from transfusion in patients awaiting primary kidney transplant
Abstract
Background: Sensitization to human leukocyte antigen (HLA) from red blood cell (RBC) transfusion is poorly quantified and is based on outdated, insensitive methods. The objective was to evaluate the effect of transfusion on the breadth, magnitude and specificity of HLA antibody formation using sensitive and specific methods.
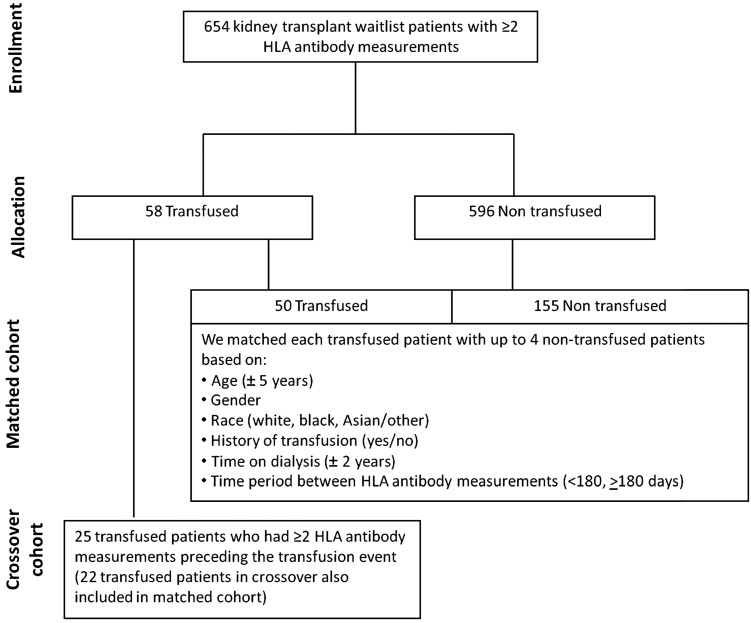
Methods: Transfusion, demographic and clinical data from the US Renal Data System were obtained for patients on dialysis awaiting primary kidney transplant who had ≥ 2 HLA antibody measurements using the Luminex single-antigen bead assay. One cohort included patients with a transfusion (n = 50) between two antibody measurements matched with up to four nontransfused patients (n = 155) by age, sex, race and vintage (time on dialysis). A second crossover cohort (n = 25) included patients with multiple antibody measurements before and after transfusion. We studied changes in HLA antibody mean fluorescence intensity (MFI) and calculated panel reactive antibody (cPRA).
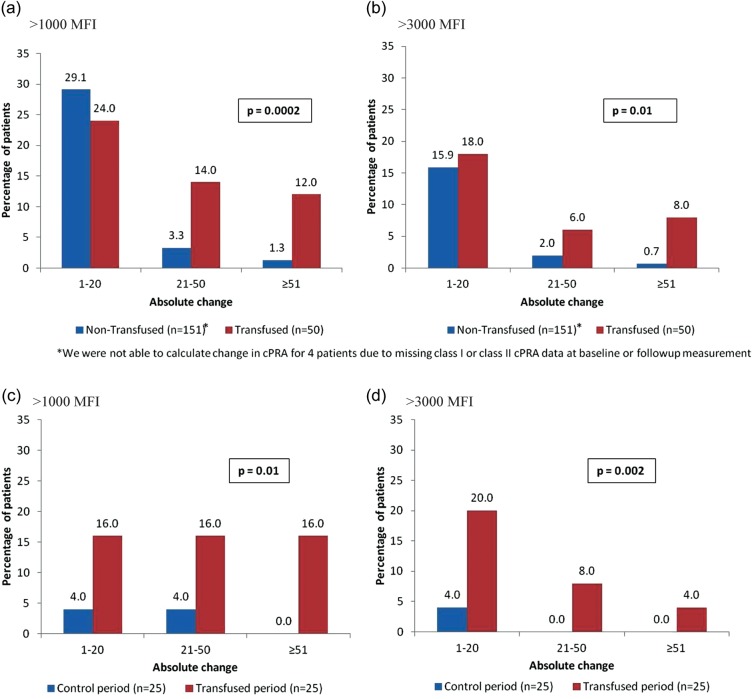
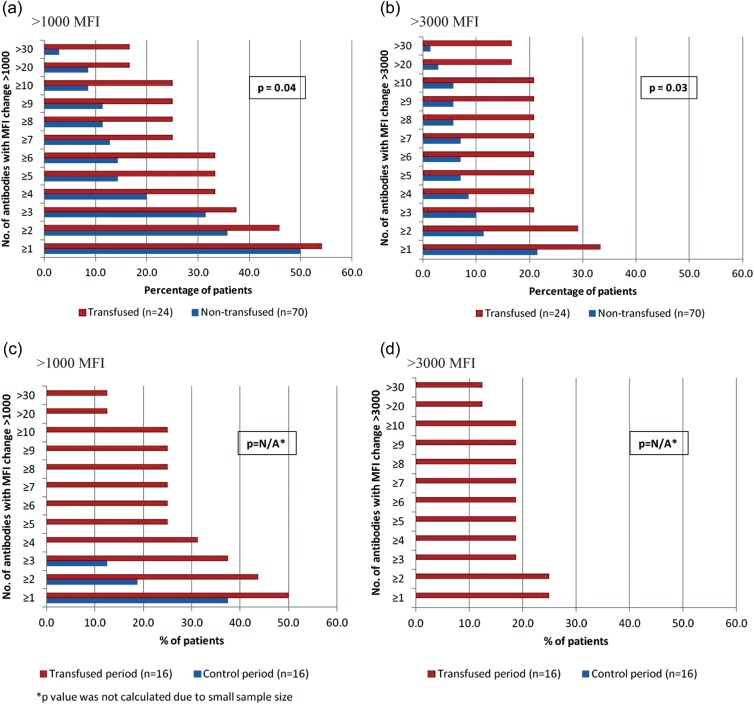
Results: In the matched cohort, 10 of 50 (20%) transfused versus 6 of 155 (4%) nontransfused patients had a ≥ 10 HLA antibodies increase of >3000 MFI (P = 0.0006); 6 of 50 (12%) transfused patients had a ≥ 30 antibodies increase (P = 0.0007). In the crossover cohort, the number of HLA antibodies increasing >1000 and >3000 MFI was higher in the transfused versus the control period, P = 0.03 and P = 0.008, respectively. Using a ≥ 3000 MFI threshold, cPRA significantly increased in both matched (P = 0.01) and crossover (P = 0.002) transfused patients.
Conclusions: Among prospective primary kidney transplant recipients, RBC transfusion results in clinically significant increases in HLA antibody strength and breadth, which adversely affect the opportunity for future transplant.
Keywords: HLA antibody; calculated panel reactive antibody; kidney transplantation; sensitization; transfusion.
Figures

Similar articles
-
Red blood cell transfusions and the risk of allosensitization in patients awaiting primary kidney transplantation.Transplantation. 2014 Mar 15;97(5):525-33. doi: 10.1097/01.tp.0000437435.19980.8f. Transplantation. 2014. PMID: 24300013
-
Effect of Single Sensitization Event on Human Leukocyte Antigen Alloimmunization in Kidney Transplant Candidates: A Single-Center Experience.Exp Clin Transplant. 2018 Feb;16(1):44-49. doi: 10.6002/ect.2016.0292. Epub 2017 Jun 28. Exp Clin Transplant. 2018. PMID: 28661314
-
Allosensitization rate of male patients awaiting first kidney grafts after leuko-depleted blood transfusion.Transplantation. 2012 Feb 27;93(4):418-22. doi: 10.1097/TP.0b013e3182419864. Transplantation. 2012. PMID: 22228416
-
Transfusion-induced HLA sensitization in wait-list patients and kidney transplant recipients.Kidney Int. 2024 Nov;106(5):795-805. doi: 10.1016/j.kint.2024.07.030. Epub 2024 Aug 22. Kidney Int. 2024. PMID: 39181398 Review.
-
Humoral Immune Response and Allograft Function in Kidney Transplantation.Am J Kidney Dis. 2015 Aug;66(2):337-47. doi: 10.1053/j.ajkd.2015.03.033. Epub 2015 May 16. Am J Kidney Dis. 2015. PMID: 25987262 Review.
Cited by
-
Harnessing the B Cell Response in Kidney Transplantation - Current State and Future Directions.Front Immunol. 2022 Jun 9;13:903068. doi: 10.3389/fimmu.2022.903068. eCollection 2022. Front Immunol. 2022. PMID: 35757745 Free PMC article. Review.
-
Anemia in Pediatric Kidney Transplant Recipients-Etiologies and Management.Front Pediatr. 2022 Jun 20;10:929504. doi: 10.3389/fped.2022.929504. eCollection 2022. Front Pediatr. 2022. PMID: 35795334 Free PMC article. Review.
-
Robotic bilateral nephrectomy for large polycystic kidney disease.BJUI Compass. 2023 Jun 24;4(6):701-708. doi: 10.1002/bco2.263. eCollection 2023 Nov. BJUI Compass. 2023. PMID: 37818019 Free PMC article.
-
Association between red blood cells transfusion and 28-day mortality rate in septic patients with concomitant chronic kidney disease.Sci Rep. 2024 Oct 10;14(1):23769. doi: 10.1038/s41598-024-75643-3. Sci Rep. 2024. PMID: 39390059 Free PMC article.
-
ESRD Payment Reform: First Do No Harm.J Am Soc Nephrol. 2016 Oct;27(10):2924-2926. doi: 10.1681/ASN.2016020153. Epub 2016 Mar 29. J Am Soc Nephrol. 2016. PMID: 27026369 Free PMC article. No abstract available.
References
-
- Port FK, Wolfe RA, Mauger EA, et al. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA. 1993;270:1339–1343. - PubMed
-
- Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725–1730. - PubMed
-
- Lee AJ, Morgan CL, Conway P, et al. Characterisation and comparison of health-related quality of life for patients with renal failure. Curr Med Res Opin. 2005;21:1777–1783. - PubMed
-
- US Renal Data System. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2012. USRDS 2012 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, Vol. 2, Chapter 10.
-
- Network OPTN. Scientific Registry of Transplant Recipients: OPTN: Data 2011. http://optn.transplant.hrsa.gov/ (September 2012, date last accessed)
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
