

Blood utilization after primary total joint arthroplasty in a large hospital network
- PMID: 24009534
- PMCID: PMC3757482
- DOI: 10.1007/s11420-013-9327-y
Blood utilization after primary total joint arthroplasty in a large hospital network
Abstract
Background: Since a study in orthopedic hip fracture patients demonstrated that a liberal hemoglobin (Hb) threshold does not improve patient morbidity and mortality relative to a restrictive Hb threshold, the standard of care in total joint arthroplasty (TJA) should be examined to understand the variability of red blood cell (RBC) transfusion following TJA.
Questions/purposes: The study aimed to answer the following questions: (1) What is the blood utilization rate after primary TJA for individual surgeons within a large hospital network? (2) What is the comparison of hospital charges, length of stay (LOS), and discharge locations among TJA patients who were and were not transfused?
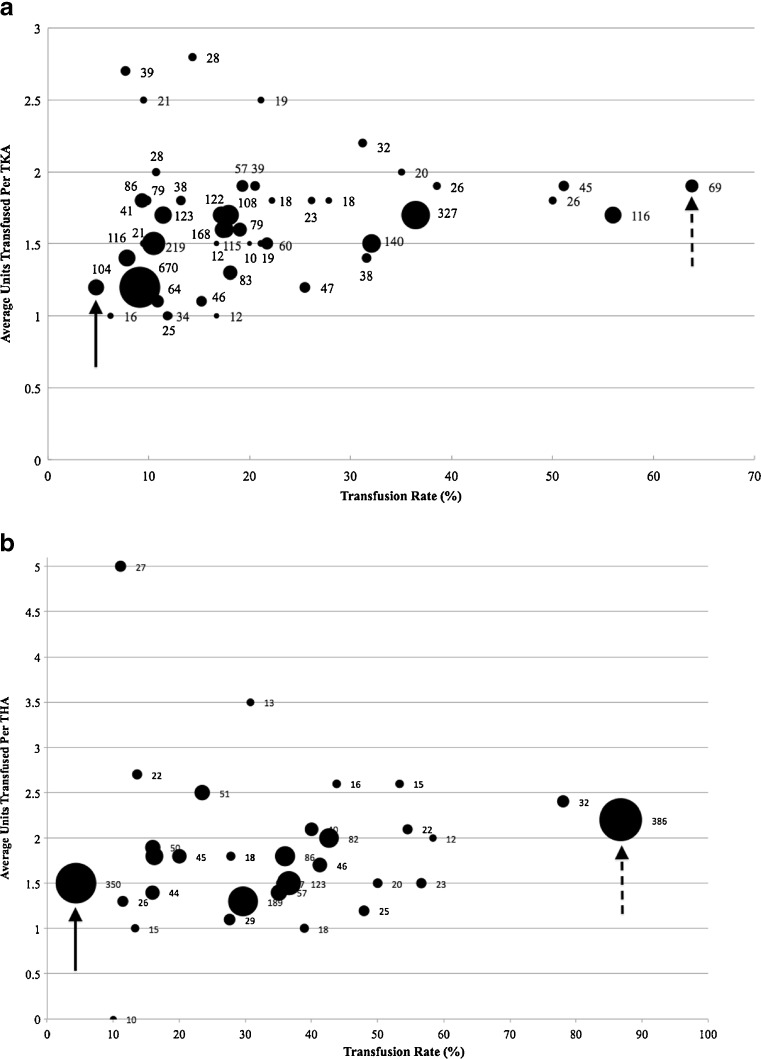
Methods: A retrospective study was conducted on 3,750 primary total knee arthroplasties (TKAs) and 2,070 primary total hip arthroplasties (THAs), and data was retrospectively collected over a 15-month period on the number of RBCs transfused per patient, along with demographic and cost details. The number of patients who received at least 1 RBC unit and the number of RBCs transfused per patient was calculated and stratified by surgeon.
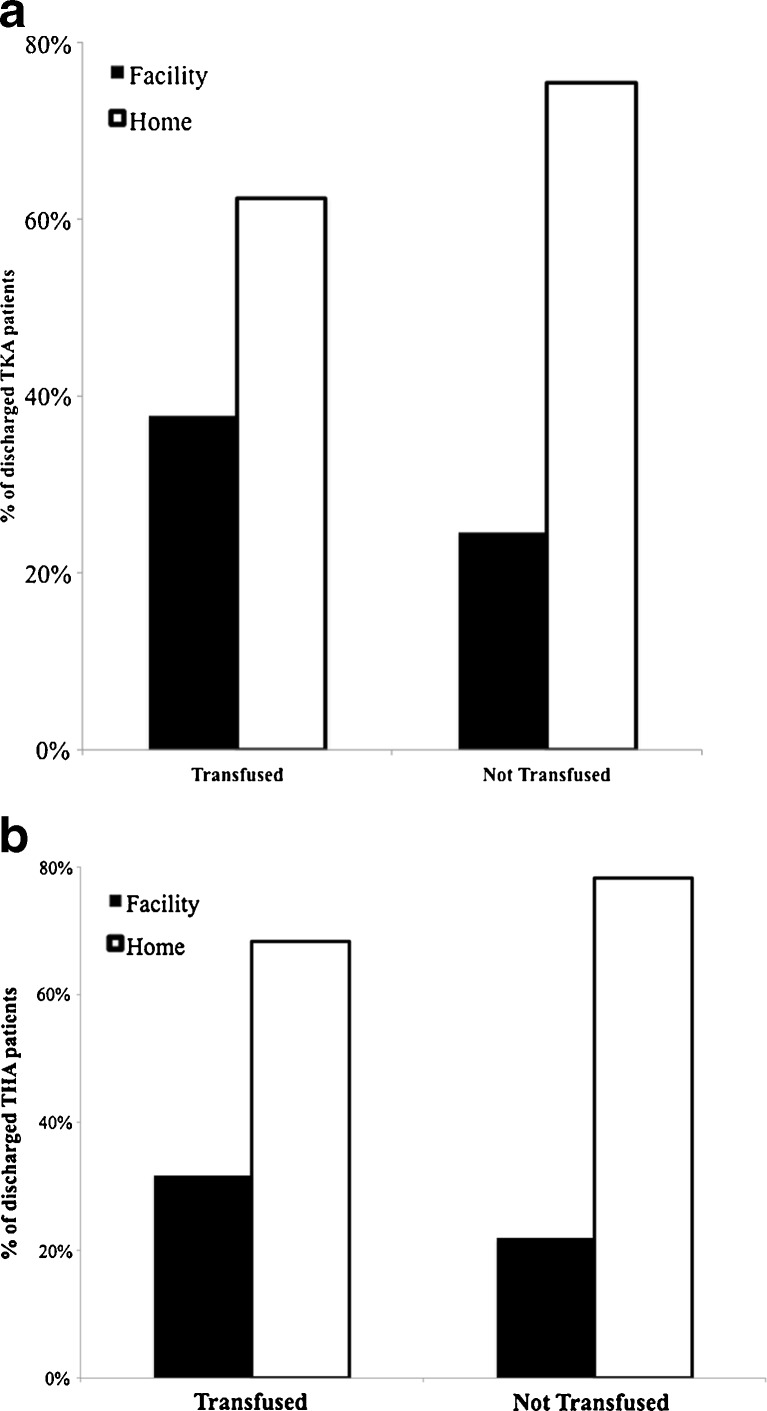
Results: In the postoperative period, 19.3% TKA patients and 38.5% THA patients received a RBC transfusion. Transfusion rates following TJA varied widely between surgeons (TKA 4.8-63.8%, THA 4.3-86.8%). Transfused TKA patients received an average of 1.65 ± 0.03 RBCs, and THA patients received an average of 1.97 ± 0.14 RBCs. LOS and hospital charges for blood transfusion patients were higher than nontransfused patients.
Conclusion: Blood utilization after primary TJA varies greatly among surgeons, suggesting that resources may be misallocated. These findings highlight the need to standardize RBC transfusion practice following TJA.
Keywords: blood management; blood utilization; intervention; red blood cell (RBC) transfusion; total joint arthroplasty; transfusion rate.
Figures

References
-
- Adams R, Lundy J. Anesthesia in cases of poor surgical risk: some suggestions for decreasing the risk. Surg Gynecol Obstet. 1942;64:1011–1019.
-
- Bernard AC, Davenport DL, Chang PK, Vaughan TB, Zwischenberger JB. Intraoperative transfusion of 1 U to 2 U packed red blood cells is associated with increased 30-day mortality, surgical-site infection, pneumonia, and sepsis in general surgery patients. J Am Coll Surg. 2009;208:931-937, 937 e931-932; discussion 938-939. - PubMed
-
- Bracey AW, Radovancevic R, Riggs SA, Houston S, Cozart H, Vaughn WK, Radovancevic B, McAllister HA, Jr, Cooley DA. Lowering the hemoglobin threshold for transfusion in coronary artery bypass procedures: effect on patient outcome. Transfusion. 1999;39:1070–1077. doi: 10.1046/j.1537-2995.1999.39101070.x. - DOI - PubMed
-
- Carless PA, Henry DA, Carson JL, Hebert PP, McClelland B, Ker K. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2010:CD002042. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
