

Hyperkalemic cardioplegia for adult and pediatric surgery: end of an era?
- PMID: 24009586
- PMCID: PMC3755226
- DOI: 10.3389/fphys.2013.00228
Hyperkalemic cardioplegia for adult and pediatric surgery: end of an era?
Abstract
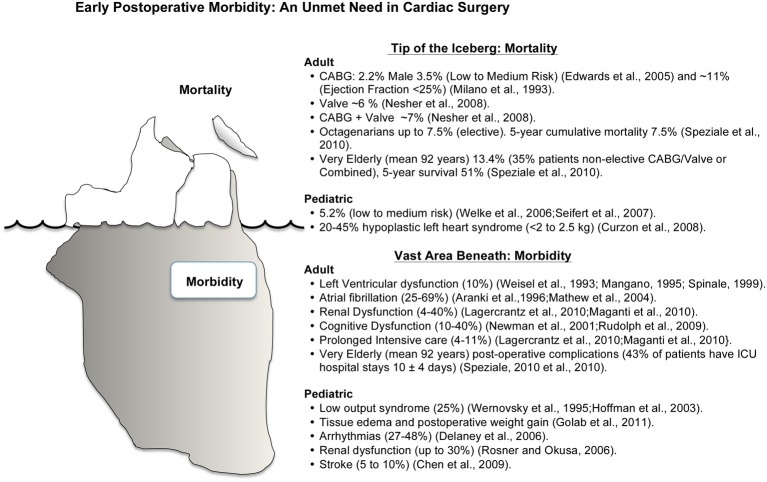
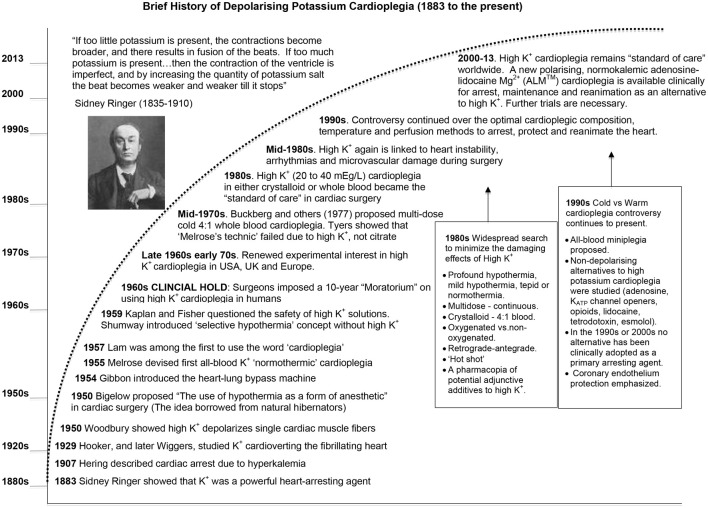
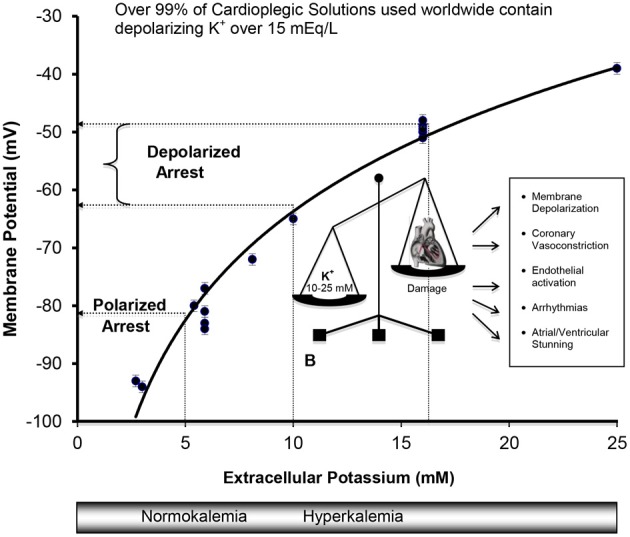
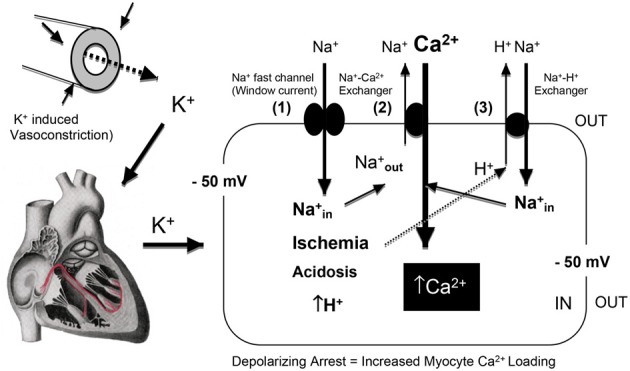
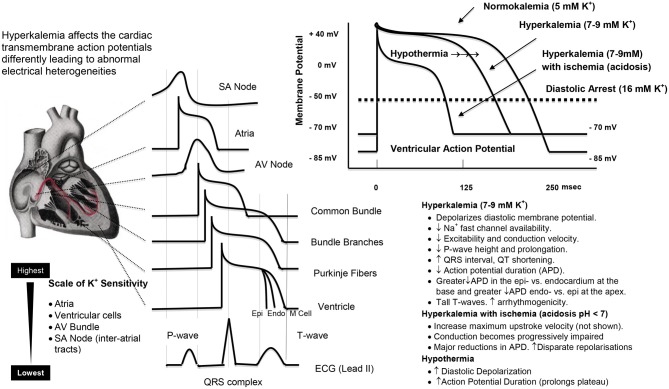
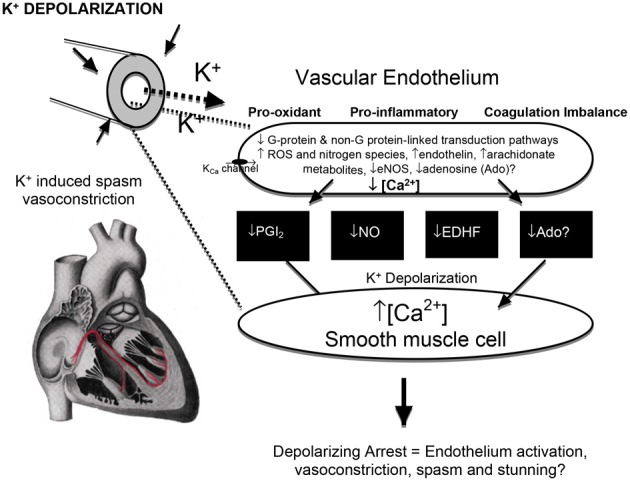
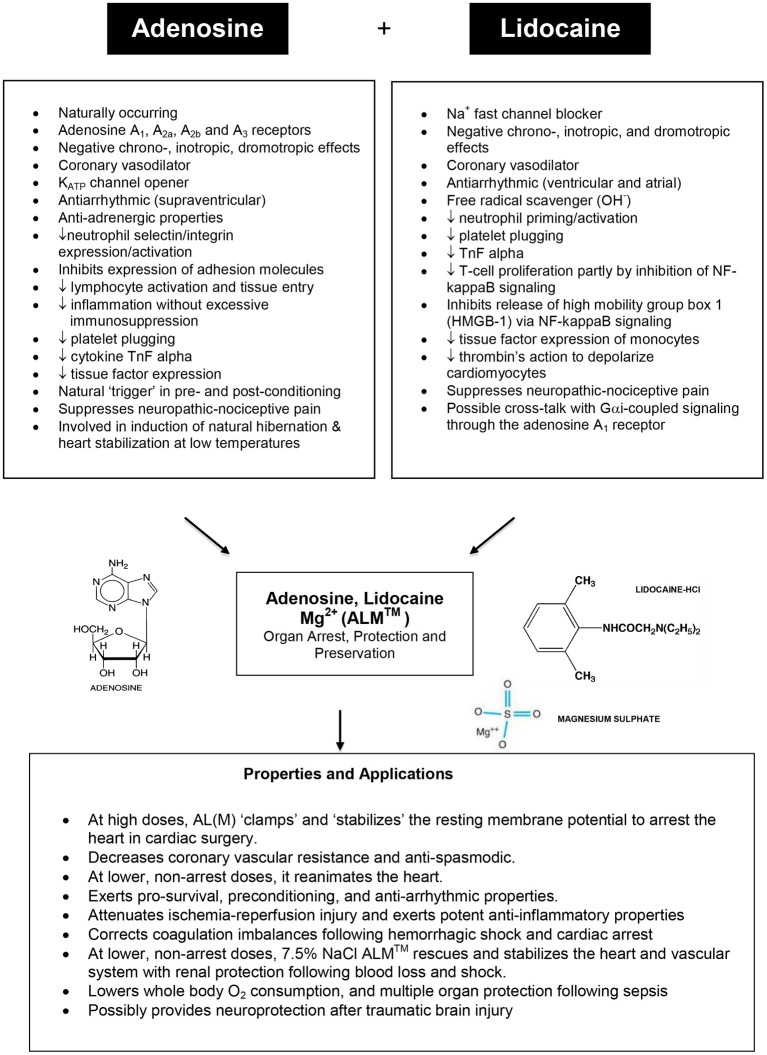
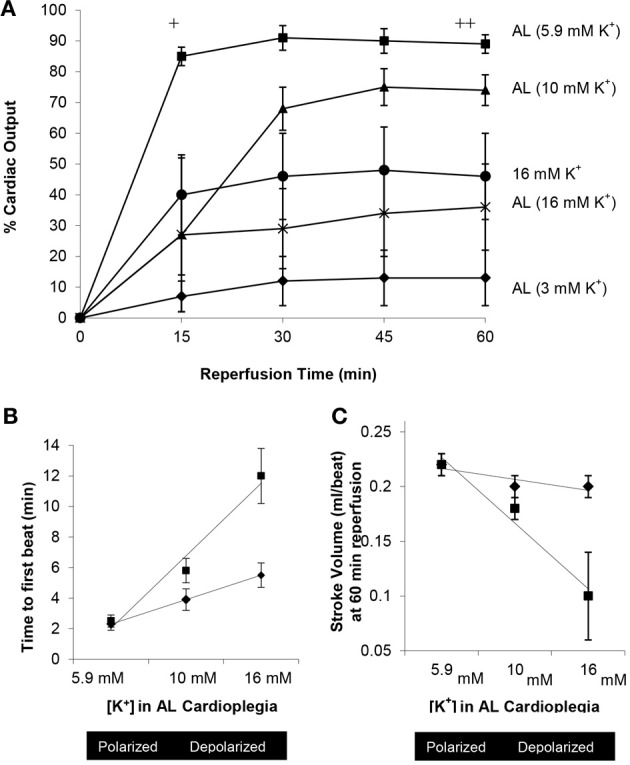
Despite surgical proficiency and innovation driving low mortality rates in cardiac surgery, the disease severity, comorbidity rate, and operative procedural difficulty have increased. Today's cardiac surgery patient is older, has a "sicker" heart and often presents with multiple comorbidities; a scenario that was relatively rare 20 years ago. The global challenge has been to find new ways to make surgery safer for the patient and more predictable for the surgeon. A confounding factor that may influence clinical outcome is high K(+) cardioplegia. For over 40 years, potassium depolarization has been linked to transmembrane ionic imbalances, arrhythmias and conduction disturbances, vasoconstriction, coronary spasm, contractile stunning, and low output syndrome. Other than inducing rapid electrochemical arrest, high K(+) cardioplegia offers little or no inherent protection to adult or pediatric patients. This review provides a brief history of high K(+) cardioplegia, five areas of increasing concern with prolonged membrane K(+) depolarization, and the basic science and clinical data underpinning a new normokalemic, "polarizing" cardioplegia comprising adenosine and lidocaine (AL) with magnesium (Mg(2+)) (ALM™). We argue that improved cardioprotection, better outcomes, faster recoveries and lower healthcare costs are achievable and, despite the early predictions from the stent industry and cardiology, the "cath lab" may not be the place where the new wave of high-risk morbid patients are best served.
Keywords: cardiac surgery; cardioplegia; endothelium; heart; history; hyperkalemia; ischemia; potassium.
Figures
References
-
- Alexander J. H., Granger C. B., Sadowski Z., Aylward P. E., White H. D., Thompson T. D., et al. (1999). Prophylactic lidocaine use in acute myocardial infarction: incidence and outcomes from two international trials. The GUSTO-I and GUSTO-IIb investigators. Am. Heart J. 137, 799–805 10.1016/S0002-8703(99)70402-3 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous