

Prevention of chronic kidney disease and subsequent effect on mortality: a systematic review and meta-analysis
- PMID: 24009665
- PMCID: PMC3756976
- DOI: 10.1371/journal.pone.0071784
Prevention of chronic kidney disease and subsequent effect on mortality: a systematic review and meta-analysis
Abstract
Objectives: To perform a systematic review of randomized controlled trials to determine whether prevention or slowing of progression of chronic kidney disease would translate into improved mortality, and if so, the attributable risk due to CKD itself on mortality.
Background: CKD is associated with increased mortality. This association is largely based on evidence from the observational studies and evidence from randomized controlled trials is lacking.
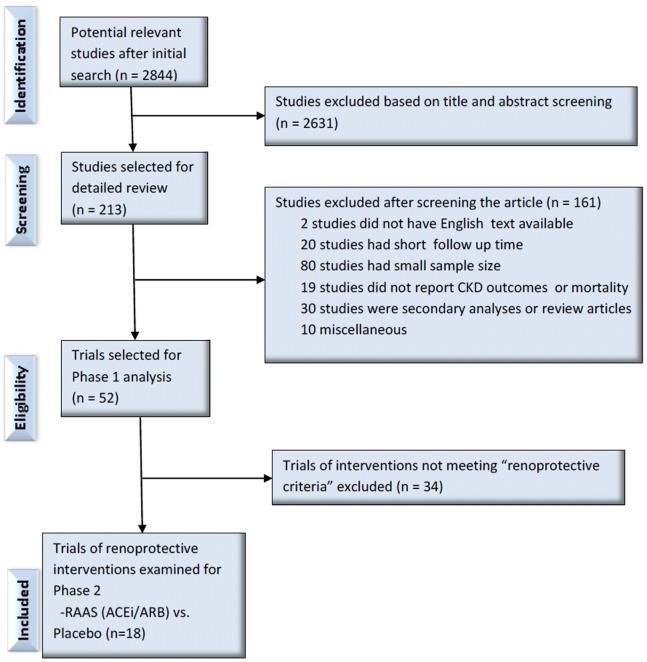
Methods: We searched Ovid, Medline and Embase for RCTs in which an intervention was given to prevent or slow the progression of CKD and mortality was reported as primary, secondary or adverse outcomes were eligible and selected. For the first phase, pooled relative risks for renal endpoints were assessed. For the second phase, we assessed the effect on mortality in trials of interventions that definitively reduced CKD endpoints.
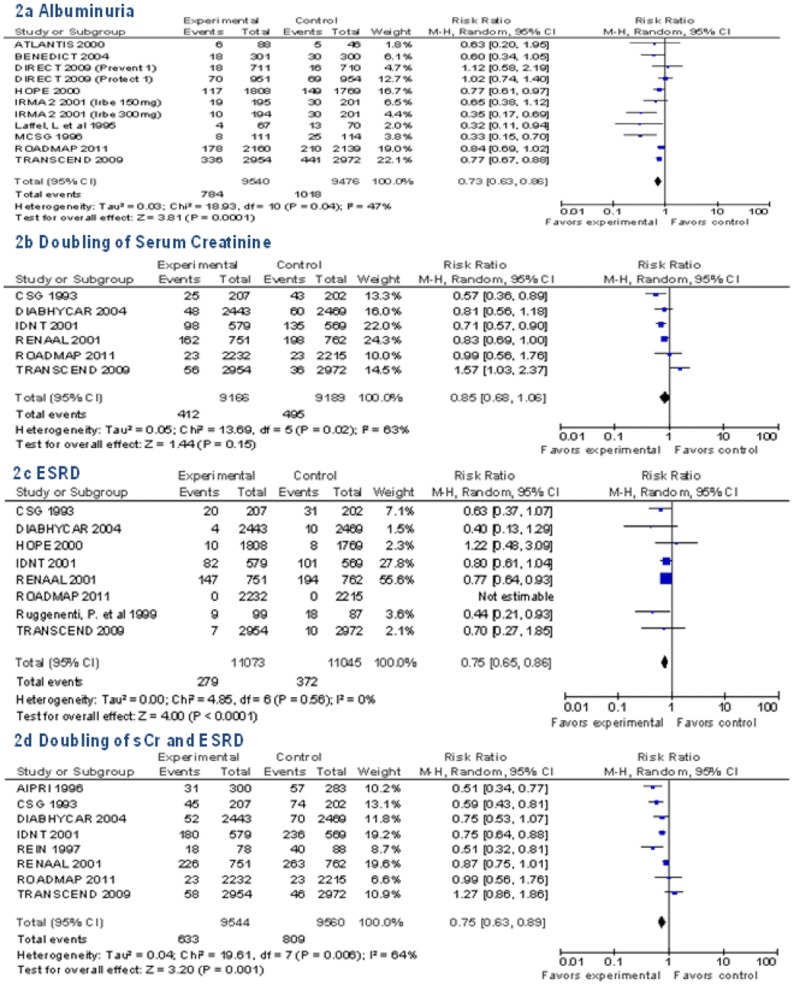
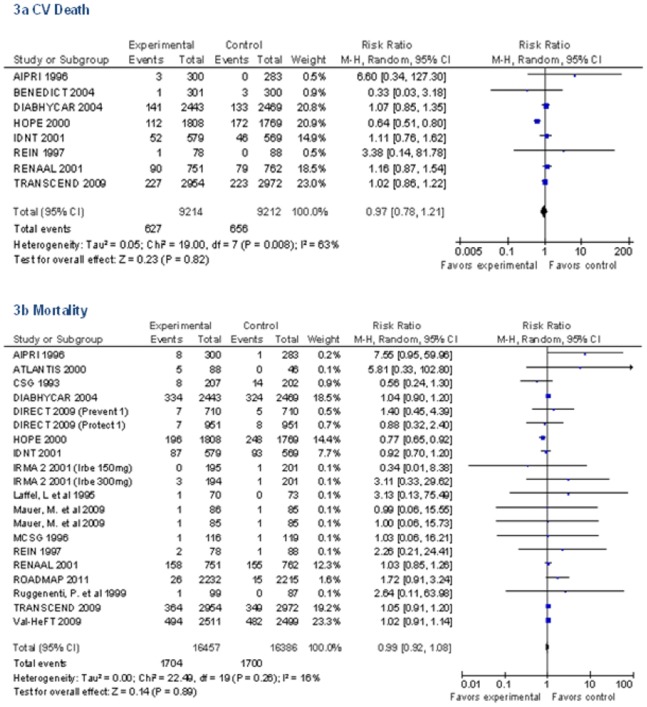
Results: Among 52 studies selected in first phase, only renin-angiotensin-aldosterone-system blockade vs. placebo (n = 18 trials, 32,557 participants) met the efficacy criteria for further analysis in the second phase by reducing renal endpoints 15 to 27% compared to placebo. There was no difference in all-cause mortality (RR 0.99, 95% CI 0.92 to 1.08) or CV death (RR 0.97, 95% CI 0.78 to 1.21) between the treatment and control groups in these trials. There was sufficient statistical power to detect a 9% relative risk reduction in all-cause mortality and a 14% relative risk reduction in cardiovascular mortality.
Conclusions: Firm evidence is lacking that prevention of CKD translates into reductions in mortality. Larger trials with longer follow-up time are needed to determine the benefit of CKD prevention on survival.
Conflict of interest statement
Figures
References
-
- CDC (2007) Prevalence of chronic kidney disease and associated risk factors–United States, 1999–2004. MMWR Morb Mortal Wkly Rep 56: 161–165. - PubMed
-
- NKF (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39: S1–266. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY (2004) Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305. - PubMed
-
- Ruilope LM, Salvetti A, Jamerson K, Hansson L, Warnold I, et al. (2001) Renal function and intensive lowering of blood pressure in hypertensive participants of the hypertension optimal treatment (HOT) study. J Am Soc Nephrol 12: 218–225. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
