

Impact of vaccination on 14 high-risk HPV type infections: a mathematical modelling approach
- PMID: 24009669
- PMCID: PMC3756967
- DOI: 10.1371/journal.pone.0072088
Impact of vaccination on 14 high-risk HPV type infections: a mathematical modelling approach
Abstract
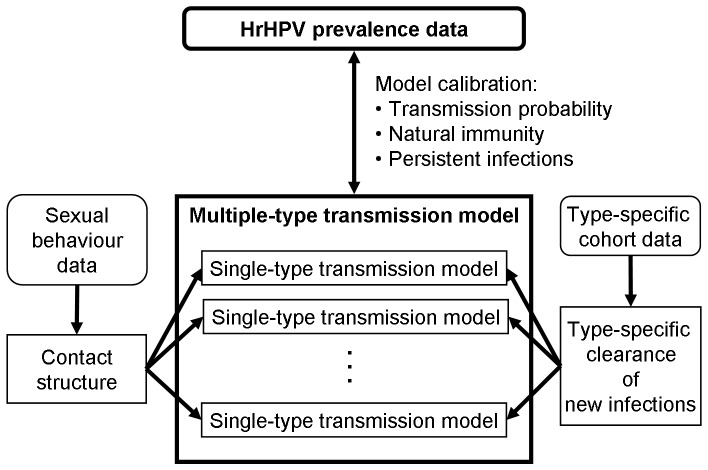
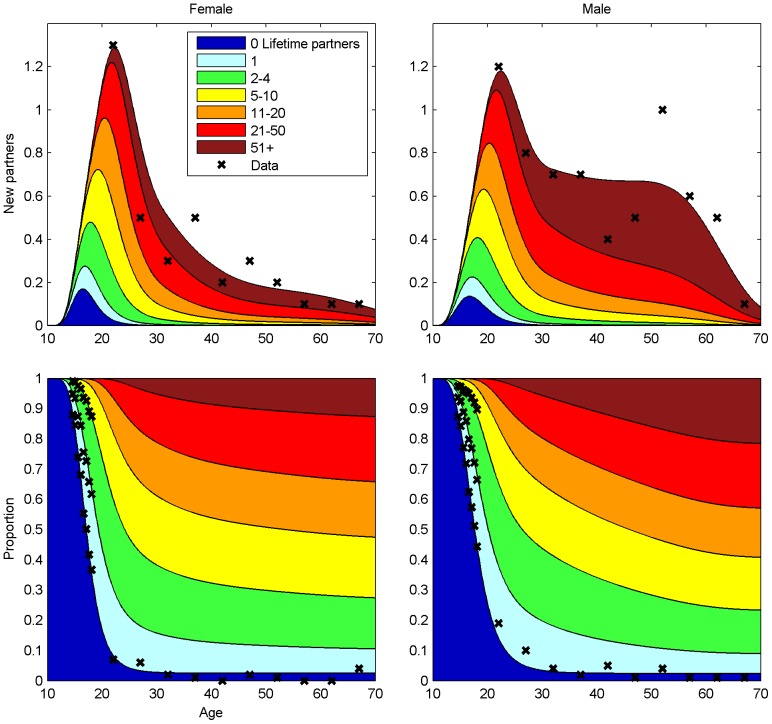
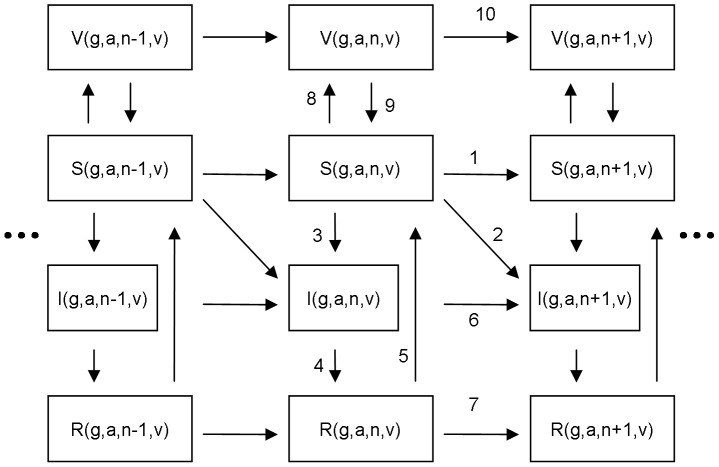
The development of high-risk human papillomavirus (hrHPV) infection to cervical cancer is a complicated process. We considered solely hrHPV infections, thus avoiding the confounding effects of disease progression, screening, and treatments. To analyse hrHPV epidemiology and to estimate the overall impact of vaccination against infections with hrHPVs, we developed a dynamic compartmental transmission model for single and multiple infections with 14 hrHPV types. The infection-related parameters were estimated using population-based sexual behaviour and hrHPV prevalence data from Finland. The analysis disclosed the important role of persistent infections in hrHPV epidemiology, provided further evidence for a significant natural immunity, and demonstrated the dependence of transmission probability estimates on the model structure. The model predicted that vaccinating girls at 80% coverage will result in a 55% reduction in the overall hrHPV prevalence and a higher 65% reduction in the prevalence of persistent hrHPV infections in females. In males, the reduction will be 42% in the hrHPV prevalence solely by the herd effect from the 80% coverage in girls. If such high coverage among girls is not reached, it is still possible to reduce the female hrHPV prevalence indirectly by the herd effect if also boys are included in the vaccination program. On the other hand, any herd effects in older unvaccinated cohorts were minor. Limiting the epidemiological model to infection yielded improved understanding of the hrHPV epidemiology and of mechanisms with which vaccination impacts on hrHPV infections.
Conflict of interest statement
Figures

Similar articles
-
Estimating the clinical benefits of vaccinating boys and girls against HPV-related diseases in Europe.BMC Cancer. 2013 Jan 8;13:10. doi: 10.1186/1471-2407-13-10. BMC Cancer. 2013. PMID: 23298365 Free PMC article.
-
Modelling the population-level impact of vaccination on the transmission of human papillomavirus type 16 in Australia.Sex Health. 2007 Sep;4(3):147-63. doi: 10.1071/sh07042. Sex Health. 2007. PMID: 17931528
-
Prevalence of genital HPV infections and HPV serology in adolescent girls, prior to vaccination.Cancer Epidemiol. 2012 Dec;36(6):519-24. doi: 10.1016/j.canep.2012.07.006. Epub 2012 Aug 17. Cancer Epidemiol. 2012. PMID: 22906483
-
Human papillomavirus vaccination and the role of herd effects in future cancer control planning: a review.Expert Rev Vaccines. 2018 May;17(5):395-409. doi: 10.1080/14760584.2018.1471986. Epub 2018 May 21. Expert Rev Vaccines. 2018. PMID: 29715059 Review.
-
Gender-neutrality, herd effect and resilient immune response for sustainable impact of HPV vaccination.Curr Opin Obstet Gynecol. 2015 Oct;27(5):326-32. doi: 10.1097/GCO.0000000000000208. Curr Opin Obstet Gynecol. 2015. PMID: 26308204 Review.
Cited by
-
Reduction in Vaccine HPV Type Infections in a Young Women Group (18-25 Years) Five Years after HPV Vaccine Introduction in Colombia.Cancer Prev Res (Phila). 2022 Jan;15(1):55-66. doi: 10.1158/1940-6207.CAPR-21-0063. Epub 2021 Oct 5. Cancer Prev Res (Phila). 2022. PMID: 34610993 Free PMC article.
-
Analysis of cervical HPV infections among unvaccinated young adult women to inform vaccine strategies in this age group: the Costa Rica HPV Vaccine Trial.Sex Transm Infect. 2022 Jul 16;99(3):180-6. doi: 10.1136/sextrans-2022-055434. Online ahead of print. Sex Transm Infect. 2022. PMID: 35842229 Free PMC article.
-
Differing Age-Specific Cervical Cancer Incidence Between Different Types of Human Papillomavirus: Implications for Predicting the Impact of Elimination Programs.Am J Epidemiol. 2021 Apr 6;190(4):506-514. doi: 10.1093/aje/kwaa121. Am J Epidemiol. 2021. PMID: 32639531 Free PMC article.
-
Effectiveness of various human papillomavirus vaccination strategies: A community randomized trial in Finland.Cancer Med. 2021 Nov;10(21):7759-7771. doi: 10.1002/cam4.4299. Epub 2021 Sep 27. Cancer Med. 2021. PMID: 34581025 Free PMC article. Clinical Trial.
-
Does Male Circumcision Reduce Women's Risk of Sexually Transmitted Infections, Cervical Cancer, and Associated Conditions?Front Public Health. 2019 Jan 31;7:4. doi: 10.3389/fpubh.2019.00004. eCollection 2019. Front Public Health. 2019. PMID: 30766863 Free PMC article.
References
-
- Dillner J, Kjaer SK, Wheeler CM, Sigurdsson K, Iversen OE, et al. (2010) Four year efficacy of prophylactic human papillomavirus quadrivalent vaccine against low grade cervical, vulvar, and vaginal intraepithelial neoplasia and anogenital warts: randomised controlled trial. BMJ 341: c3493. - PMC - PubMed
-
- Lehtinen M, Paavonen J, Wheeler CM, Jaisamrarn U, Garland SM, et al. (2012) Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol 13: 89–99. - PubMed
-
- Munoz N, Kjaer SK, Sigurdsson K, Iversen OE, Hernandez-Avila M, et al. (2010) Impact of human papillomavirus (HPV)-6/11/16/18 vaccine on all HPV-associated genital diseases in young women. J Natl Cancer Inst 102: 325–339. - PubMed
-
- Wheeler CM, Castellsague X, Garland SM, Szarewski A, Paavonen J, et al. (2012) Cross-protective efficacy of HPV-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by non-vaccine oncogenic HPV types: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol 13: 100–110. - PubMed
-
- Wheeler CM, Kjaer SK, Sigurdsson K, Iversen OE, Hernandez-Avila M, et al. (2009) The impact of quadrivalent human papillomavirus (HPV; types 6, 11, 16, and 18) L1 virus-like particle vaccine on infection and disease due to oncogenic nonvaccine HPV types in sexually active women aged 16–26 years. J Infect Dis 199: 936–944. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
