

A randomized trial of two coverage targets for mass treatment with azithromycin for trachoma
- PMID: 24009792
- PMCID: PMC3757067
- DOI: 10.1371/journal.pntd.0002415
A randomized trial of two coverage targets for mass treatment with azithromycin for trachoma
Abstract
Background: The World Health Organization recommends at least 3 annual antibiotic mass drug administrations (MDA) where the prevalence of trachoma is > 10% in children ages 1-9 years, with coverage at least at 80%. However, the additional value of higher coverage targeted at children with multiple rounds is unknown.
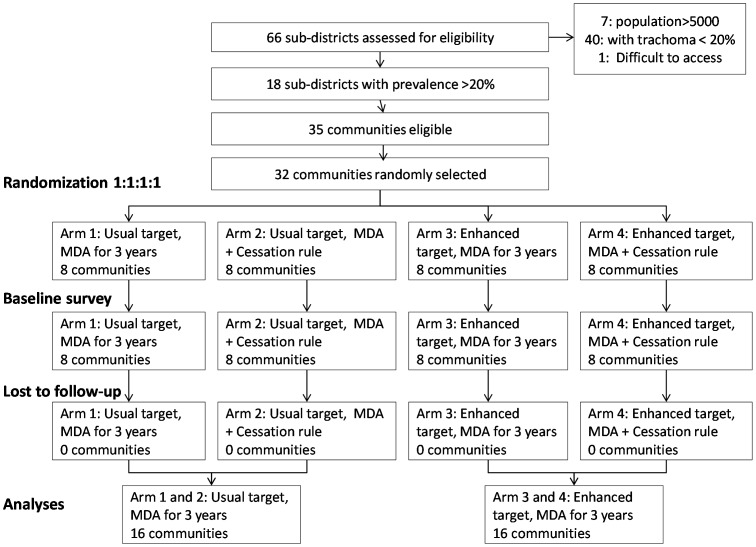
Trial design: 2 × 2 factorial community randomized, double blind, trial.
Trial methods: 32 communities with prevalence of trachoma ≥ 20% were randomized to: annual MDA aiming for coverage of children between 80%-90% (usual target) versus aiming for coverag e> 90% (enhanced target); and to: MDA for three years versus a rule of cessation of MDA early if the estimated prevalence of ocular C. trachomatis infection was less than 5%. The primary outcome was the community prevalence of infection with C. trachomatis at 36 months.
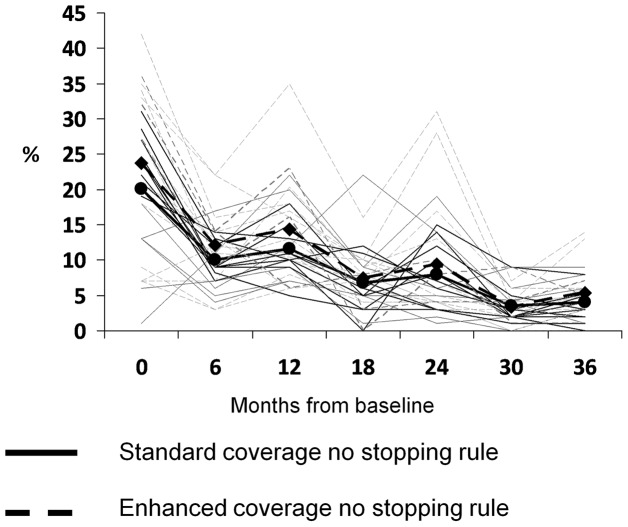
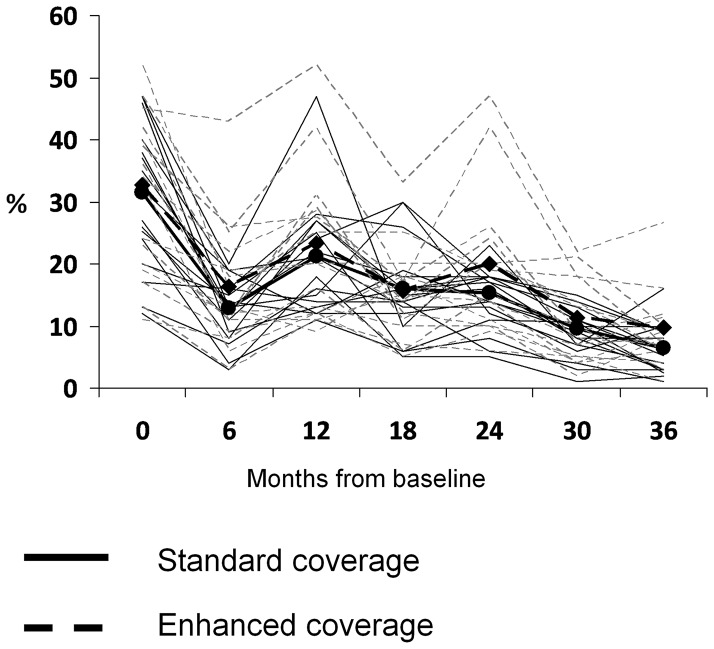
Results: Over the trial's course, no community met the MDA cessation rule, so all communities had the full 3 rounds of MDA. At 36 months, there was no significant difference in the prevalence of infection, 4.0 versus 5.4 (mean adjusted difference = 1.4%, 95% CI = -1.0% to 3.8%), nor in the prevalence of trachoma, 6.1 versus 9.0 (mean adjusted difference = 2.6%, 95% CI = -0.3% to 5.3%) comparing the usual target to the enhanced target group. There was no difference if analyzed using coverage as a continuous variable.
Conclusion: In communities that had pre-treatment prevalence of follicular trachoma of 20% or greater, there is no evidence that MDA can be stopped before 3 annual rounds, even with high coverage. Increasing coverage in children above 90% does not appear to confer additional benefit.
Conflict of interest statement
I have read the journal's policy and have no conflicts. Azithromycin was donated to the Government of Tanzania through the Trachoma donation program at Pfizer International and managed by International Trachoma Initiative. Pfizer and ITI had no role in the design, conduct, data collection, management, interpretation of the data, or decision to submit the paper for publication.
Figures
References
-
- Mariotti S, Pascolini D, Rose-Nussbaumer J (2009) Trachoma: Global Magnitude of a preventable cause of blindness. Br J Ophthalmol 93: 563–568. - PubMed
-
- Frick KD, Basilion EV, Hanson CL, Colchero MA (2003) Estimating the burden and economic impact of trachomatous visual loss. Ophthalmic Epidemiol 10: 121–132. - PubMed
-
- West SK (2004) Trachoma: new assault on an ancient disease. Prog Retin Eye Res 23: 381–401. - PubMed
-
- Solomon AW, Holland MJ, Burton MJ, et al. (2003) Strategies for control of trachoma: observational study with quantitative PCR. Lancet 362: 198–204. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
