

Evaluation of femoral tunnel positioning using 3-dimensional computed tomography and radiographs after single bundle anterior cruciate ligament reconstruction with modified transtibial technique
- PMID: 24009904
- PMCID: PMC3758988
- DOI: 10.4055/cios.2013.5.3.188
Evaluation of femoral tunnel positioning using 3-dimensional computed tomography and radiographs after single bundle anterior cruciate ligament reconstruction with modified transtibial technique
Abstract
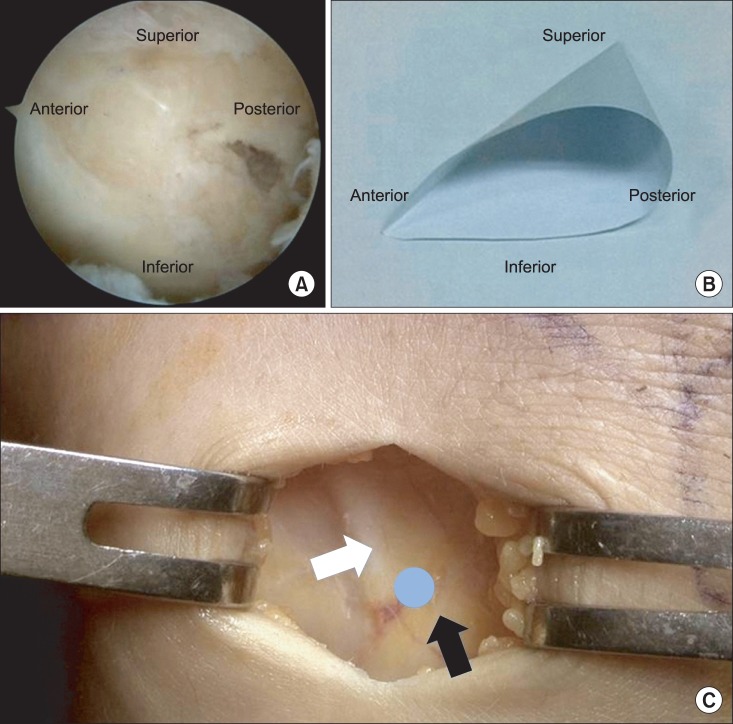
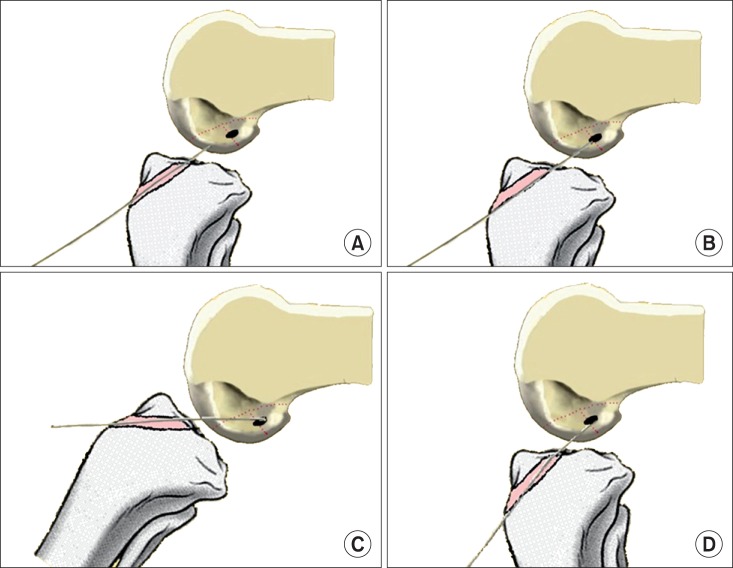
Background: The purpose of this study is to report a modified transtibial technique to approach the center of anatomical femoral footprint in anterior cruciate ligament (ACL) reconstruction and to investigate the accurate femoral tunnel position with 3-dimensional computed tomography (3D-CT) and radiography after reconstruction.
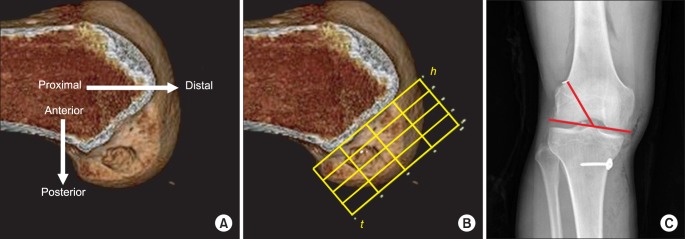
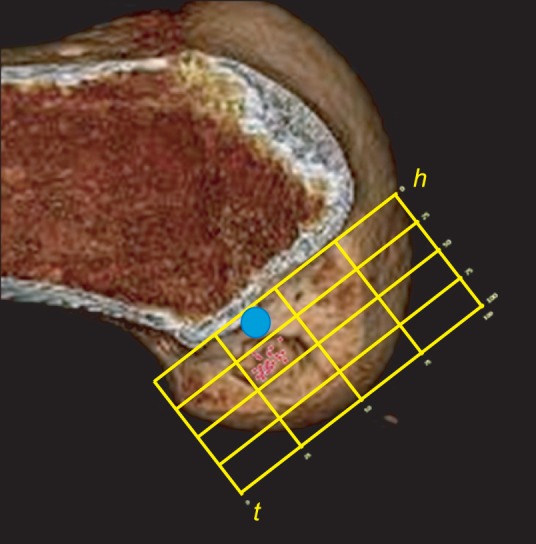
Methods: From December 2010 to October 2011, we evaluated 98 patients who underwent primary ACL reconstruction using a modified transtibial technique to approach the center of anatomical femoral footprint in single bundle ACL reconstruction with hamstring autograft. Their femoral tunnel positions were investigated with 3D-CT and radiography postoperatively. Femoral tunnel angle was measured on the postoperative anteroposterior (AP) radiograph and the center of the femoral tunnel aperture on the lateral femoral condyle was assessed with 3D-CT according to the quadrant method by two orthopedic surgeons.
Results: According to the quadrant method with 3D-CT, the femoral tunnel was measured at a mean of 32.94% ± 5.16% from the proximal condylar surface (parallel to the Blumensaat line) and 41.89% ± 5.58% from the notch roof (perpendicular to the Blumensaat line) with good interobserver (intraclass correlation coefficients [ICC], 0.766 and 0.793, respectively) and intraobserver reliability (ICC, 0.875 and 0.893, respectively). According to the radiographic measurement on the AP view, the femoral tunnel angles averaged 50.43° ± 7.04° (ICC, 0.783 and 0.911, respectively).
Conclusions: Our modified transtibial technique is anticipated to provide more anatomical placement of the femoral tunnel during ACL reconstruction than the former traditional transtibial techniques.
Keywords: 3-Dimensional computed tomography; Anterior cruciate ligament reconstruction; Femoral tunnel; Transtibial technique.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Aglietti P, Giron F, Buzzi R, Biddau F, Sasso F. Anterior cruciate ligament reconstruction: bone-patellar tendon-bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J Bone Joint Surg Am. 2004;86(10):2143–2155. - PubMed
-
- Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o'clock and 10 o'clock femoral tunnel placement. 2002 Richard O'Connor Award paper. Arthroscopy. 2003;19(3):297–304. - PubMed
-
- Bedi A, Raphael B, Maderazo A, Pavlov H, Williams RJ., 3rd Transtibial versus anteromedial portal drilling for anterior cruciate ligament reconstruction: a cadaveric study of femoral tunnel length and obliquity. Arthroscopy. 2010;26(3):342–350. - PubMed
-
- Garofalo R, Mouhsine E, Chambat P, Siegrist O. Anatomic anterior cruciate ligament reconstruction: the two-incision technique. Knee Surg Sports Traumatol Arthrosc. 2006;14(6):510–516. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
