

Erdheim-Chester Disease: a comprehensive review of the literature
- PMID: 24011030
- PMCID: PMC3849848
- DOI: 10.1186/1750-1172-8-137
Erdheim-Chester Disease: a comprehensive review of the literature
Abstract
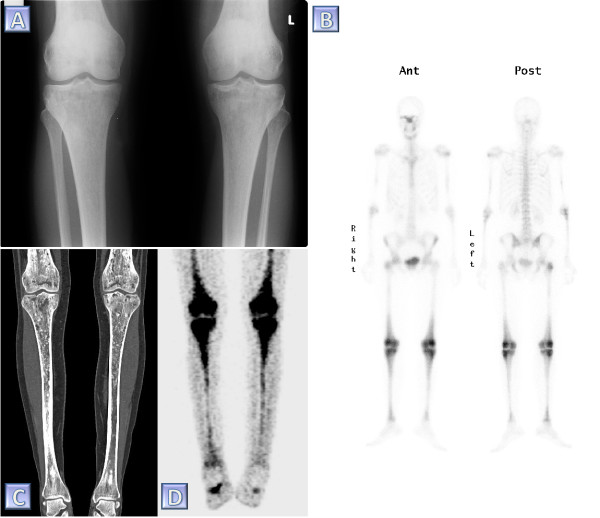
Erdheim-Chester Disease (ECD) is a rare form of non Langerhans' cell histiocytosis. Individuals affected by this disease are typically adults between their 5th and 7th decades of life. Males and females are almost equally affected. The multi systemic form of ECD is associated with significant morbidity, which may arise due to histiocytic infiltration of critical organ systems. Among the more common sites of involvement are the skeleton, central nervous system, cardiovascular system, lungs, kidneys (retroperitoneum) and skin. The most common presenting symptom of ECD is bone pain. The etiology of ECD is unknown yet thought to be associated with an intense TH1 immune response. It may also be associated with the V600E BRAF mutation, as described in as many as half of the patients in recent studies. Bilateral symmetric increased tracer uptake on 99mTc bone scintigraphy affecting the periarticular regions of the long bones is highly suggestive of ECD. However, definite diagnosis of ECD is established only once CD68(+), CD1a(-) histiocytes are identified within a biopsy specimen. At present, this obscure ailment embodies numerous challenges to medical science. Given its rarity, it is diagnostically elusive and requires a high level of clinical suspicion. Therapeutically, it is of limited alternatives. Currently, interferon-α is the most extensively studied agent in the treatment of ECD and serves as the first line of treatment. Treatment with other agents is based on anecdotal case reports and on the basis of biological rationale. Nevertheless, cladribine (2CDA), anakinra and vemurafenib are currently advocated as promising second line treatments for patients whose response to interferon-α is unsatisfactory. Overall, the 5 year survival of ECD is 68%. Herein, the authors mustered and brought about a panoramic consolidation of all the relevant facts regarding ECD. This work highlights the different clinical, radiological and pathological manifestations associated with ECD, the differential diagnoses, the various treatment options and the acknowledged science explaining the disease.
Figures
References
-
- Arnaud L, Hervier B, Neel A, Hamidou MA, Kahn JE, Wechsler B, Perez-Pastor G, Blomberg B, Fuzibet JG, Dubourguet F. et al.CNS involvement and treatment with interferon-alpha are independent prognostic factors in Erdheim-Chester disease: a multicenter survival analysis of 53 patients. Blood. 2011;117:2778–2782. - PubMed
-
- Haroche J, Arnaud L, Amoura Z. Erdheim-Chester disease. Curr Opin Rheumatol. 2012;24:53–59. - PubMed
-
- Carpinteri R, Patelli I, Casanueva FF, Giustina A. Pituitary tumours: inflammatory and granulomatous expansive lesions of the pituitary. Best Pract Res Clin Endocrinol Metab. 2009;23:639–650. - PubMed
-
- Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D, Wechsler J, Brun B, Remy M, Wallaert B, Petit H, Grimaldi A, Wechsler B, Godeau P. Erdheim-Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine. 1996;75:157–169. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
