

Longitudinal spectral domain optical coherence tomography changes in eyes with intraocular lymphoma
- PMID: 24011267
- PMCID: PMC3847273
- DOI: 10.1186/1869-5760-3-59
Longitudinal spectral domain optical coherence tomography changes in eyes with intraocular lymphoma
Abstract
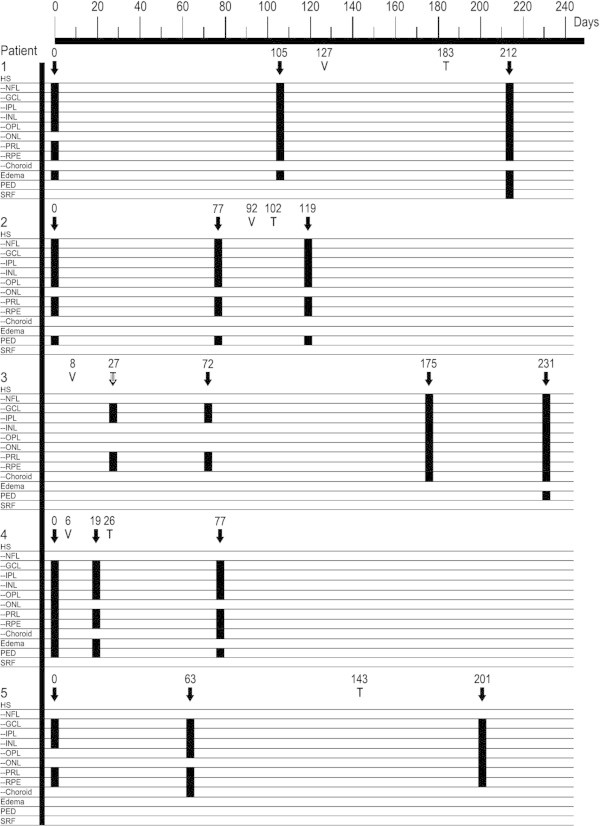
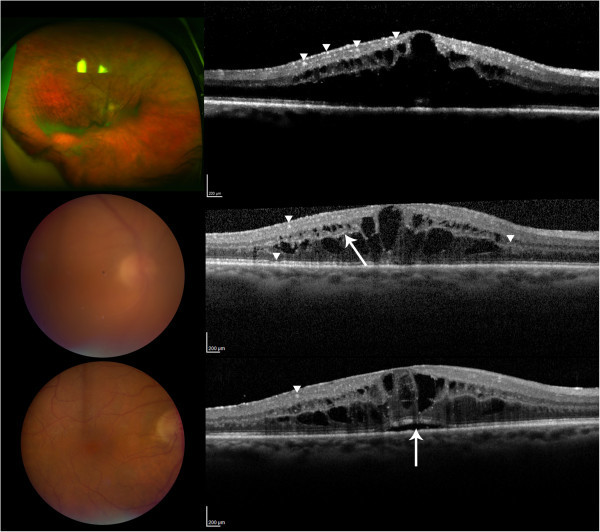
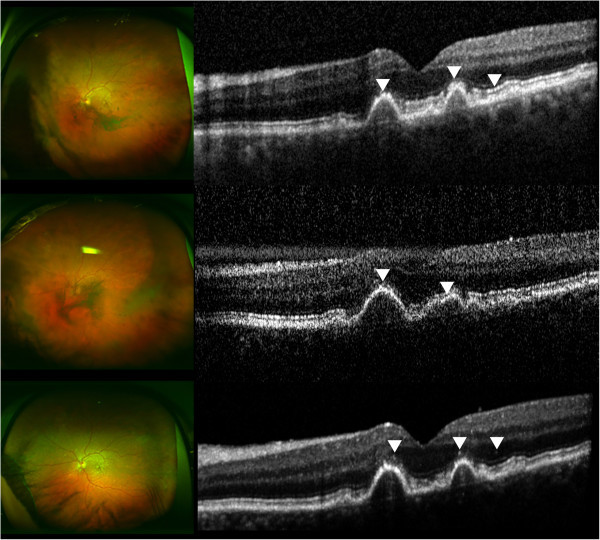
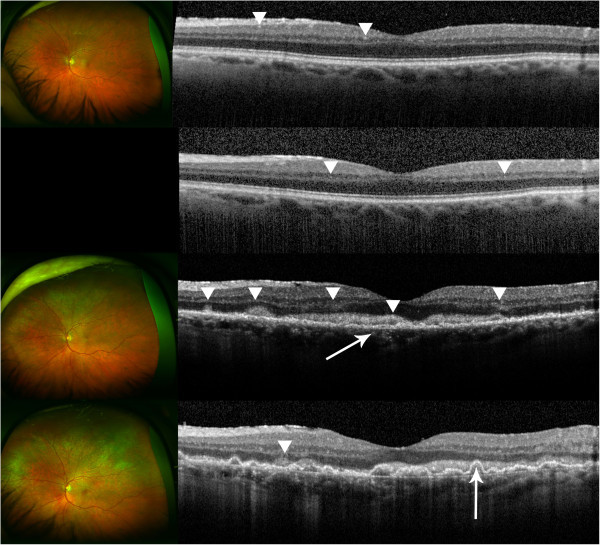
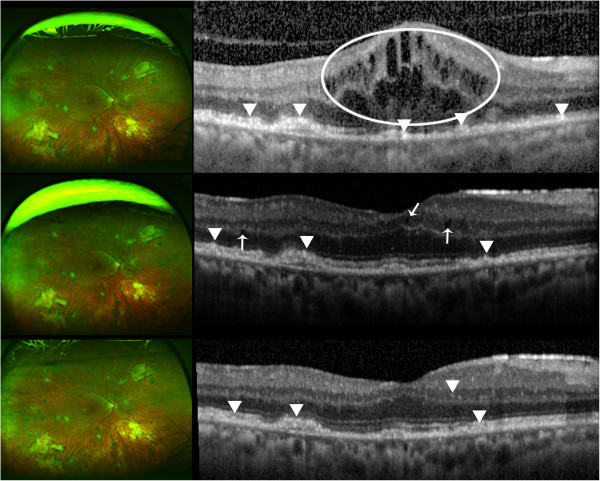
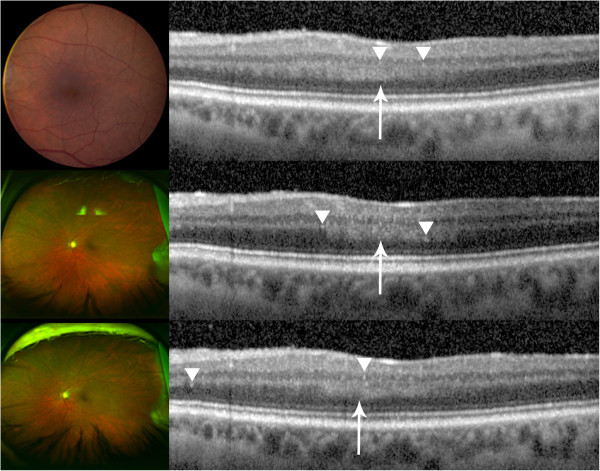
Background: Cases of patients with primary intraocular lymphoma (PIOL) were retrospectively analyzed to describe the longitudinal intra-retinal morphological changes in PIOL as visualized on images obtained by spectral domain optical coherence tomography (SD-OCT).
Results: In a retrospective case series, Heidelberg Spectralis SD-OCT images obtained in the longitudinal evaluation of patients with biopsy-proven PIOL were analyzed and assessed. The images were graded for the presence of macular edema (ME), pigment epithelial detachment (PED), subretinal fluid (SRF), and hyperreflective signals. SD-OCT scans of five eyes from five patients were assessed. Patients showed signs of inflammation, such as ME and SRF, which were resolved with treatments in some cases. Hyperreflective signals were found in all eyes in the form of nodules or bands across the retina, with the highest frequency of appearance in the ganglion cell layer, inner plexiform layer, photoreceptor layer, and retinal pigment epithelium; such signals increased with the progression of PIOL.
Conclusion: SD-OCT may be employed to monitor the progression of PIOL. Hyperreflective signals on OCT may correspond with increase in disease activities, along with other findings such as ME, PED, and SRF.
Figures
References
-
- Bardenstein DS. Intraocular lymphoma. Cancer Control. 1998;3(4):317–325. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
