

Comparison of graft patency, limb salvage, and antithrombotic therapy between prosthetic and autogenous below-knee bypass for critical limb ischemia
- PMID: 24011814
- PMCID: PMC4279244
- DOI: 10.1016/j.avsg.2013.01.019
Comparison of graft patency, limb salvage, and antithrombotic therapy between prosthetic and autogenous below-knee bypass for critical limb ischemia
Abstract
Background: The autogenous vein is the preferred conduit in below-knee vascular reconstructions. However, many argue that prosthetic grafts can perform well in crural bypass with adjunctive antithrombotic therapy. We therefore compared outcomes of below-knee prosthetic versus autologous vein bypass grafts for critical limb ischemia and the use of adjunctive antithrombotic therapy in both settings.
Methods: Utilizing the registry of the Vascular Study Group of New England (2003-2009), we studied 1227 patients who underwent below-knee bypass for critical limb ischemia, 223 of whom received a prosthetic graft to the below-knee popliteal artery (70%) or more distal target (30%). We used propensity matching to identify a patient cohort receiving single-segment saphenous vein yet had remained similar to the prosthetic cohort in terms of characteristics, graft origin/target, and antithrombotic regimen. Main outcome measures were graft patency and major limb amputation within 1 year. Secondary outcomes were bleeding complications (reoperation or transfusion) and mortality. We performed comparisons by conduit type and by antithrombotic therapy.
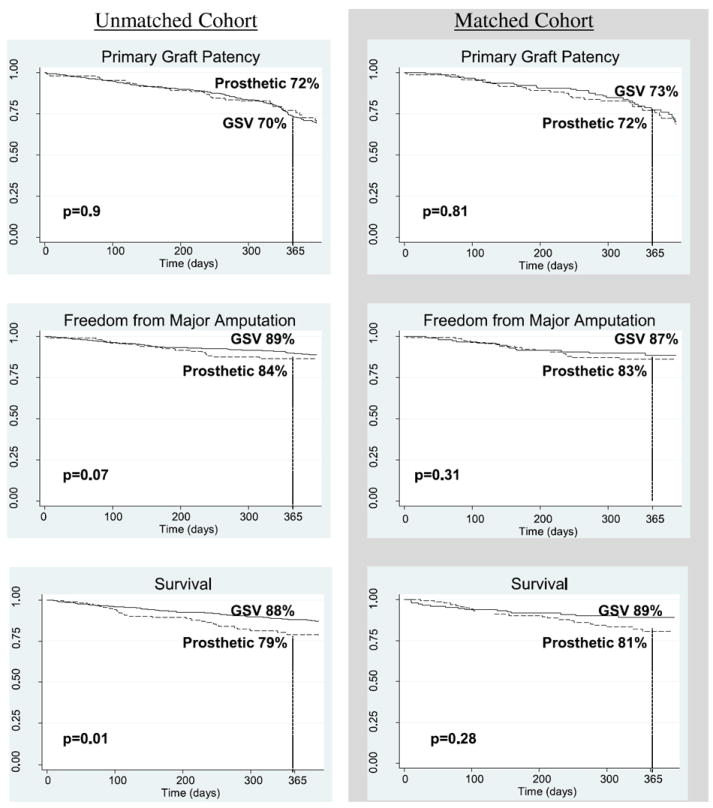
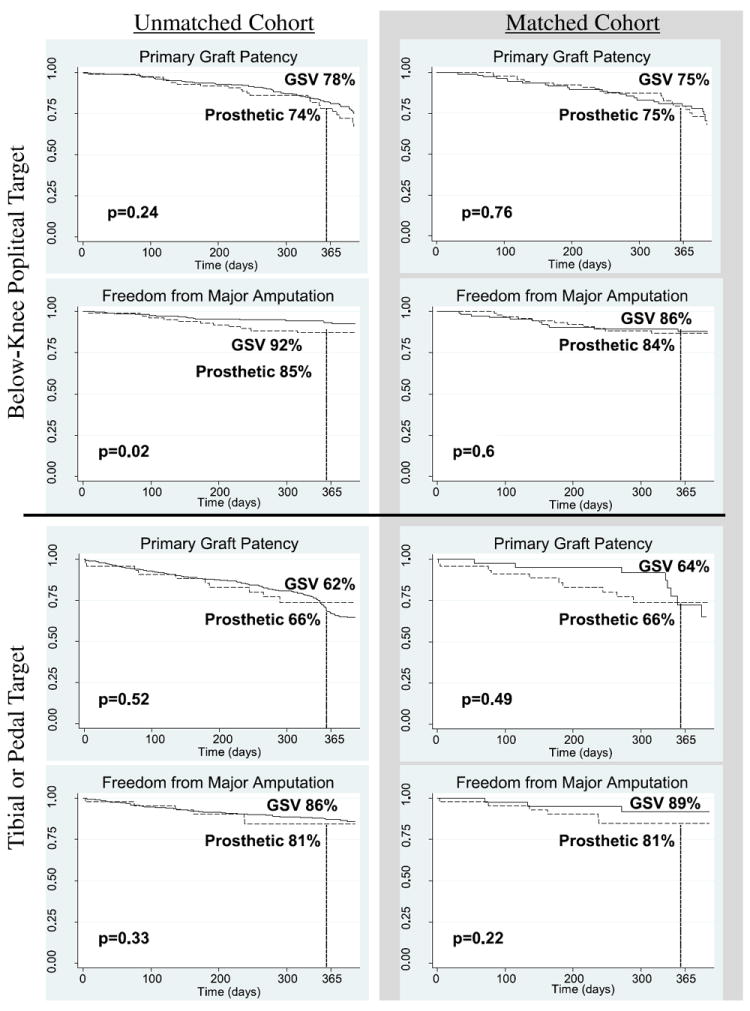
Results: Patients receiving prosthetic conduit were more likely to be treated with warfarin than those with greater saphenous vein (57% vs. 24%, P<0.001). After propensity score matching, we found no significant difference in primary graft patency (72% vs. 73%, P=0.81) or major amputation rates (17% vs. 13%, P=0.31) between prosthetic and single-segment saphenous vein grafts. In a subanalysis of grafts to tibial versus popliteal targets, we noted equivalent primary patency and amputation rates between prosthetic and venous conduits. Whereas overall 1-year prosthetic graft patency rates varied from 51% (aspirin+clopidogrel) to 78% (aspirin+warfarin), no significant differences were seen in primary patency or major amputation rates by antithrombotic therapy (P=0.32 and 0.17, respectively). Further, the incidence of bleeding complications and 1-year mortality did not differ by conduit type or antithrombotic regimen in the propensity-matched analysis.
Conclusions: Although limited in size, our study demonstrates that, with appropriate patient selection and antithrombotic therapy, 1-year outcomes for below-knee prosthetic bypass grafting can be comparable to those for greater saphenous vein conduit.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic) Circulation. 2006;113:e463–5. - PubMed
-
- Archie JP., Jr Femoropopliteal bypass with either adequate ipsilateral reversed saphenous vein or obligatory polytetrafluoroethylene. Ann Vasc Surg. 1994;8:475–84. - PubMed
-
- Nicoloff AD, Taylor LM, Jr, McLafferty RB, Moneta GL, Porter JM. Patient recovery after infrainguinal bypass grafting for limb salvage. J Vasc Surg. 1998;27:256–63. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) Eur J Vasc Endovasc Surg. 2007;33(Suppl. 1):S1–75. - PubMed
-
- Green RM, Abbott WM, Matsumoto T, et al. Prosthetic above-knee femoropopliteal bypass grafting: five-year results of a randomized trial. J Vasc Surg. 2000;31:417–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
