

J wave syndromes: molecular and cellular mechanisms
- PMID: 24011992
- PMCID: PMC3825797
- DOI: 10.1016/j.jelectrocard.2013.08.006
J wave syndromes: molecular and cellular mechanisms
Abstract
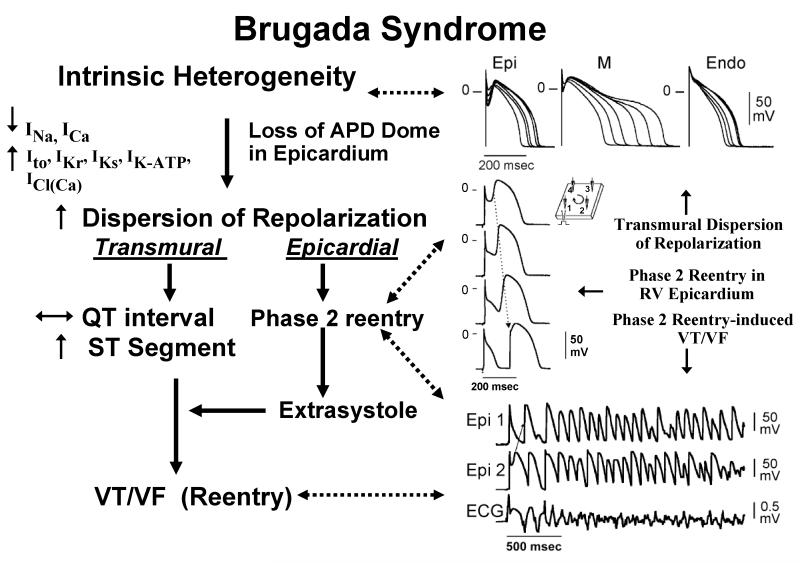
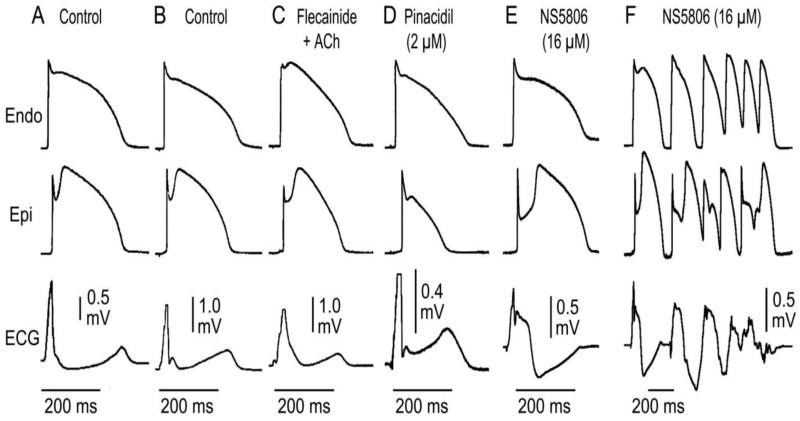
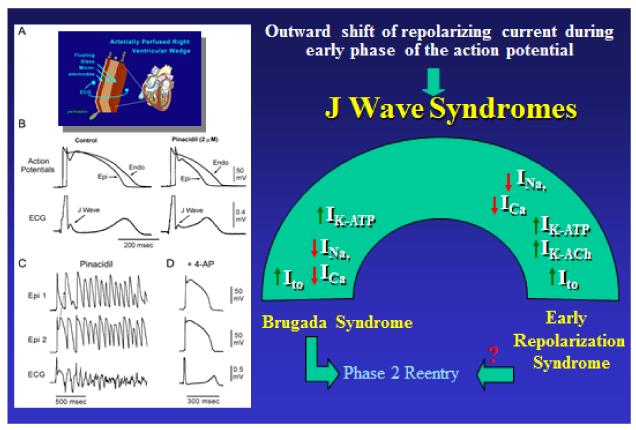
An early repolarization (ER) pattern in the ECG, consisting of J point elevation, distinct J wave with or without ST segment elevation or slurring of the terminal part of the QRS, was long considered a benign electrocardiographic manifestation. Experimental studies a dozen years ago suggested that an ER is not always benign, but may be associated with malignant arrhythmias. Validation of this hypothesis derives from recent case-control and population-based studies showing that an ER pattern in inferior or infero-lateral leads is associated with increased risk for life-threatening arrhythmias, termed early repolarization syndrome (ERS). Because accentuated J waves characterize both Brugada syndrome (BrS) and ERS, these syndromes have been grouped under the heading of J wave syndromes. BrS and ERS appear to share common ECG characteristics, clinical outcomes, risk factors as well as a common arrhythmic platform related to amplification of Ito-mediated J waves. However, they differ with respect to the magnitude and lead location of abnormal J waves and can be considered to represent a continuous spectrum of phenotypic expression. Recent studies support the hypothesis that BrS and ERS are caused by a preferential accentuation of the AP notch in right or left ventricular epicardium, respectively, and that this repolarization defect is accentuated by cholinergic agonists. Quinidine, cilostazol and isoproterenol exert ameliorative effects by reversing these repolarization abnormalities. Identifying subjects truly at risk is the challenge ahead. Our goal here is to review the clinical and genetic aspects as well as the cellular and molecular mechanisms underlying the J wave syndromes.
Keywords: Brugada syndrome; Cardiac arrhythmias; Early repolarization syndrome; Idiopathic ventricular fibrillation; Sudden cardiac death.
© 2013.
Figures
References
-
- Tomaszewski W. Changement electrocardiographiques observes chez un homme mort de froid. Arch Mal Coeur Vaiss. 1938;31:525–528.
-
- Osborn JJ. Experimental hypothermia: respiratory and blood pH changes in relation to cardiac function. Am J Physiol. 1953;175:389–398. - PubMed
-
- Clements SD, Hurst JW. Diagnostic value of ECG abnormalities observed in subjects accidentally exposed to cold. Am J Cardiol. 1972;29:729–734. - PubMed
-
- Thompson R, Rich J, Chmelik F, Nelson WL. Evolutionary changes in the electrocardiogram of severe progressive hypothermia. J Electrocardiol. 1977;10:67–70. - PubMed
-
- Eagle K. Images in clinical medicine. Osborn waves of hypothermia. N Engl J Med. 1994:10–680. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
