

Preclinical Alzheimer's disease and its outcome: a longitudinal cohort study
- PMID: 24012374
- PMCID: PMC3904678
- DOI: 10.1016/S1474-4422(13)70194-7
Preclinical Alzheimer's disease and its outcome: a longitudinal cohort study
Abstract
Background: New research criteria for preclinical Alzheimer's disease have been proposed, which include stages for cognitively normal individuals with abnormal amyloid markers (stage 1), abnormal amyloid and neuronal injury markers (stage 2), or abnormal amyloid and neuronal injury markers and subtle cognitive changes (stage 3). We aimed to investigate the prevalence and long-term outcome of preclinical Alzheimer's disease according to these criteria.
Methods: Participants were cognitively normal (clinical dementia rating [CDR]=0) community-dwelling volunteers aged at least 65 years who were enrolled between 1998 and 2011 at the Washington University School of Medicine (MO, USA). CSF amyloid-β1-42 and tau concentrations and a memory composite score were used to classify participants as normal (both markers normal), preclinical Alzheimer's disease stage 1-3, or suspected non-Alzheimer pathophysiology (SNAP, abnormal injury marker without abnormal amyloid marker). The primary outcome was the proportion of participants in each preclinical AD stage. Secondary outcomes included progression to CDR at least 0·5, symptomatic Alzheimer's disease (score of at least 0·5 for memory and at least one other domain and cognitive impairments deemed to be due to Alzheimer's disease), and mortality. We undertook survival analyses using subdistribution and standard Cox hazards models and linear mixed models.
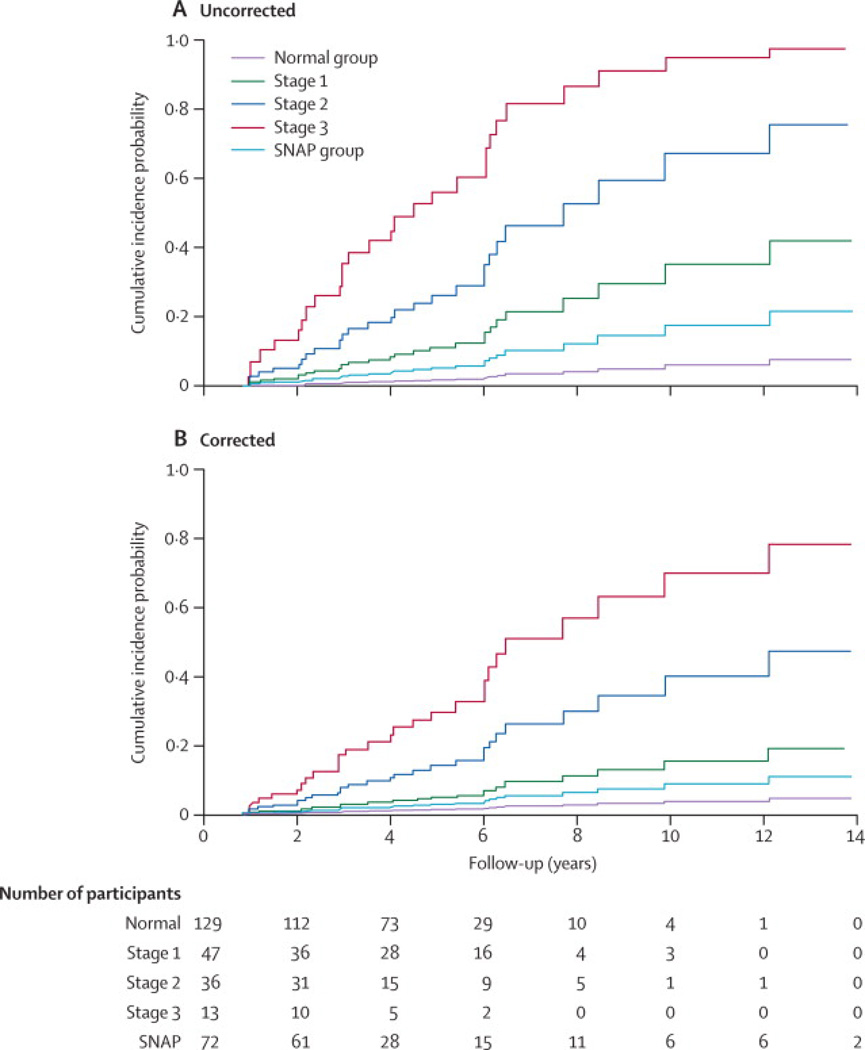
Findings: Of 311 participants, 129 (41%) were classed as normal, 47 (15%) as stage 1, 36 (12%) as stage 2, 13 (4%) as stage 3, 72 (23%) as SNAP, and 14 (5%) remained unclassified. The 5-year progression rate to CDR at least 0·5, symptomatic Alzheimer's disease was 2% for participants classed as normal, 11% for stage 1, 26% for stage 2, 56% for stage 3, and 5% for SNAP. Compared with individuals classed as normal, participants with preclinical Alzheimer's disease had an increased risk of death after adjusting for covariates (hazard ratio 6·2, 95% CI 1·1-35·0; p=0·040).
Interpretation: Preclinical Alzheimer's disease is common in cognitively normal elderly people and is associated with future cognitive decline and mortality. Thus, preclinical Alzheimer's disease could be an important target for therapeutic intervention.
Funding: National Institute of Aging of the National Institutes of Health (P01-AG003991, P50-AG05681, P01-AG02676), Internationale Stichting Alzheimer Onderzoek, the Center for Translational Molecular Medicine project LeARN, the EU/EFPIA Innovative Medicines Initiative Joint Undertaking, and the Charles and Joanne Knight Alzheimer Research Initiative.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Ms. Stephanie Vos receives research support from the Center for Translational Molecular Medicine, project LeARN (grant 02N-01) and received funds from Internationale Stichting Alzheimer Onderzoek (ISAO) to perform this study. No conflict of interest exists.
Dr. Xiong reports no disclosures.
Dr. Visser has served as an advisory board member of Bristol-Myers Squibb. He receives/received research grants from Bristol-Myers Squibb, the European Union’s 6th and 7th Framework programme, Life Sciences, Genomics and Biotechnology for Health and Innovative Medicines Initiative Joint Undertaking under grant agreement n° 115372, resources of which are composed of financial contribution from the European Union's 7th Framework programme and EFPIA companies (PJV), Diagenic, Norway, and Innogenetics, Belgium. No conflict of interest exists.
Mr. Mateusz Jasielec reports no disclosures.
Dr. Hassenstab reports no disclosures.
Dr. Grant reports no disclosures.
Dr. Cairns reports no disclosures.
Dr. Morris has participated or is currently participating in clinical trials of anti-dementia drugs sponsored by the following companies: Janssen Immunotherapy, and Pfizer. Dr. Morris has served as a consultant for the following companies: Eisai, Esteve, Janssen Alzheimer Immunotherapy Program, Glaxo-Smith-Kline, Novartis, and Pfizer. He receives research support from Eli Lilly/Avid Radiopharmaceuticals and is funded by NIH grants # P50AG005681; P01AG003991; P01AG026276 and U19AG032438. Neither Dr. Morris nor his family owns stock or has equity interest (outside of mutual funds or other externally directed accounts) in any pharmaceutical or biotechnology company. No conflict of interest exists. Dr. Holtzman reports consulting for Bristol-Myers-Squibb, AstraZeneca, and Genentech, and is on the scientific advisory board of C2N Diagnostics. His research grant support is from the NIH, Ellison Medical Foundation, Cure Alzheimer’s Fund, Pfizer, Astra Zeneca, C2N Diagnostics and Integrated Diagnostics. No conflict of interest exists.
Dr. Fagan serves as an advisory board member for Roche and Eli Lilly. No conflict of interest exists.
Figures
Comment in
-
Do preclinical Alzheimer's disease criteria work?Lancet Neurol. 2013 Oct;12(10):933-5. doi: 10.1016/S1474-4422(13)70217-5. Epub 2013 Sep 4. Lancet Neurol. 2013. PMID: 24012373 No abstract available.
-
Preclinical Alzheimer's disease criteria.Lancet Neurol. 2013 Dec;12(12):1134. doi: 10.1016/S1474-4422(13)70222-9. Epub 2013 Sep 9. Lancet Neurol. 2013. PMID: 24025450 Free PMC article. No abstract available.
References
-
- Price J, Morris JC. Tangles and plaques in non demented aging and "preclinical" Alzheimer's disease. Ann Neurol. 1999;45:358–368. - PubMed
-
- Hulette C, Welsh-Bohmer K, Murray M, Saunders A, Mash D, Mcintyre L. Neuropathological and neuropsychological changes in "normal" aging: evidence for preclinical Alzheimer disease in cognitively normal individuals. J Neuropathol Exp Neurol. 1998;57:1168–1274. - PubMed
-
- Braak H, Braak E. Frequency of stages of Alzheimer-related lesions in different age categories. Neurobiol Aging. 1997;18:351–357. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
