

Aspiration therapy leads to weight loss in obese subjects: a pilot study
- PMID: 24012983
- PMCID: PMC4025911
- DOI: 10.1053/j.gastro.2013.08.056
Aspiration therapy leads to weight loss in obese subjects: a pilot study
Abstract
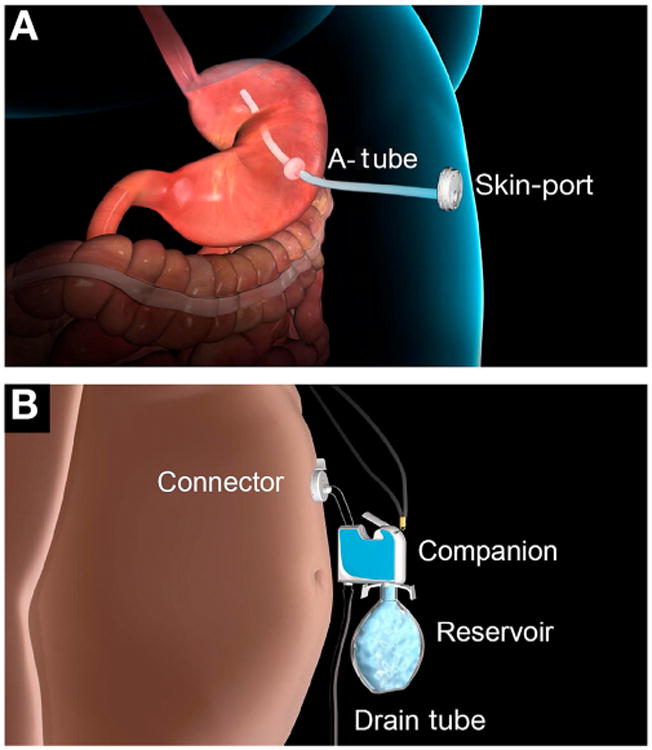
Background & aims: Obese patients rarely achieve long-term weight loss with only lifestyle interventions. We evaluated the use of endoscopic aspiration therapy for obesity. Aspiration therapy involves endoscopic placement of a gastrostomy tube (A-Tube) and the AspireAssist siphon assembly (Aspire Bariatrics, King of Prussia, PA) to aspirate gastric contents 20 minutes after meal consumption.
Methods: We performed a pilot study of 18 obese subjects who were randomly assigned (2:1) to groups that underwent aspiration therapy for 1 year plus lifestyle therapy (n = 11; mean body mass index, 42.6 ± 1.4 kg/m(2)) or lifestyle therapy only (n = 7; mean body mass index, 43.4 ± 2.0 kg/m(2)). Lifestyle intervention comprised a 15-session diet and behavioral education program.
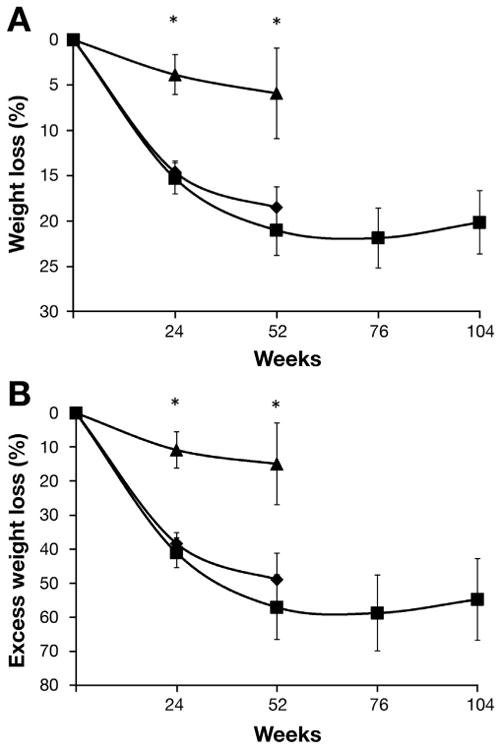
Results: Ten of the 11 subjects who underwent aspiration therapy and 4 of the 7 subjects who underwent lifestyle therapy completed the first year of the study. After 1 year, subjects in the aspiration therapy group lost 18.6% ± 2.3% of their body weight (49.0% ± 7.7% of excess weight loss [EWL]) and those in the lifestyle therapy group lost 5.9% ± 5.0% (14.9% ± 12.2% of EWL) (P < .04). Seven of the 10 subjects in the aspiration therapy group completed an additional year of therapy and maintained a 20.1% ± 3.5% body weight loss (54.6% ± 12.0% of EWL). There were no adverse effects of aspiration therapy on eating behavior and no evidence of compensation for aspirated calories with increased food intake. No episodes of binge eating in the aspiration therapy group or serious adverse were reported.
Conclusions: In a pilot study, aspiration therapy appears to be a safe and effective long-term weight loss therapy for obesity.
Trial registration: ClinicalTrials.gov NCT00773903.
Keywords: ALT; AT; BDI-II; BMI; Beck Depression Inventory; EDE; EWL; Eating Disorder Examination; Endoscopic Bariatric Therapy; LT; Obesity; Overweight; PEG; Percutaneous Endoscopic Gastrostomy; RCT; alanine aminotransferase; aspiration therapy plus lifestyle therapy; body mass index; excess weight loss; lifestyle therapy only; percutaneous endoscopic gastrostomy; randomized controlled trial.
Copyright © 2013 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

Comment in
-
Could aspiration therapy for obesity be an effective and safe alternative to traditional bariatric surgery?Gastroenterology. 2013 Dec;145(6):1188-90. doi: 10.1053/j.gastro.2013.10.038. Gastroenterology. 2013. PMID: 24409479 No abstract available.
References
-
- Flegal KM, Carroll MD, Ogden CL, et al. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303:235–241. - PubMed
-
- Finkelstein EA, Trogdon JG, Cohen JW, et al. Annual medical spending attributable to obesity: payer- and service-specific estimates. Health Aff (Millwood) 2009;28:w822–w831. - PubMed
-
- Klein S, Wadden T, Sugerman HJ. AGA technical review on obesity. Gastroenterology. 2002;123:882–932. - PubMed
-
- Foster GD, Wyatt HR, Hill JO, et al. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med. 2003;348:2082–2090. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
