

Anterior versus posterior approach for treatment of thoracolumbar burst fractures: a meta-analysis
- PMID: 24013718
- PMCID: PMC3804690
- DOI: 10.1007/s00586-013-2987-y
Anterior versus posterior approach for treatment of thoracolumbar burst fractures: a meta-analysis
Abstract
Purpose: To critically review and summarize the literature comparing the results of surgery via an anterior approach and that via a posterior approach for the treatment of thoracolumbar burst fractures to identify the better approach.
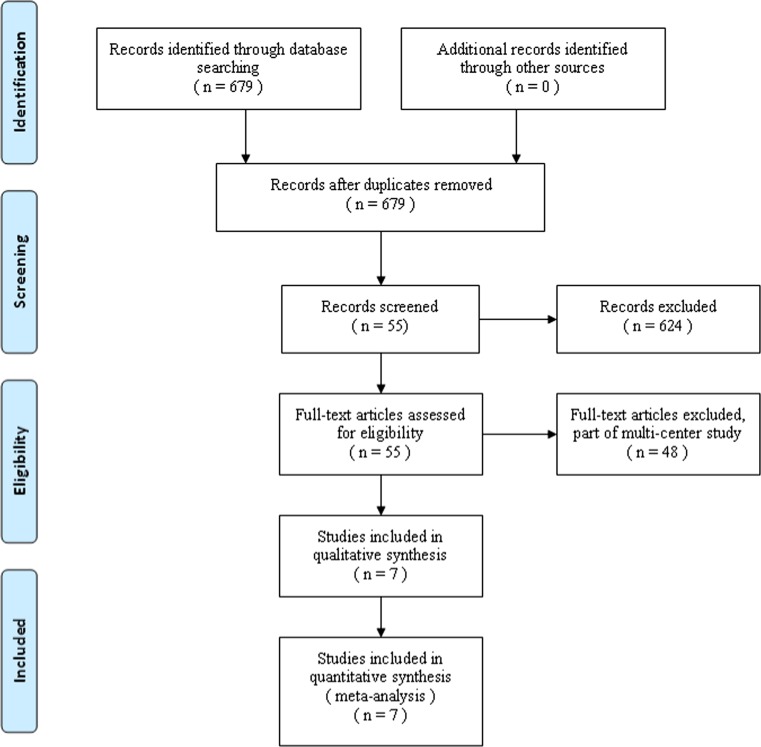
Methods: In this meta-analysis, we conducted electronic searches of MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials and other databases using the search terms "thoracolumbar fractures", "anterior", "posterior", "controlled clinical trials". Relevant journals or conference proceedings were also searched manually. Data extraction and quality assessment were in accordance with Cochrane Collaboration guidelines. The analysis was performed on individual patient data from all the trials that met the selection criteria. Sensitivity analysis was performed when there was significant heterogeneity. Results were expressed as risk difference for dichotomous outcomes and mean difference for continuous outcomes with 95 % confidence interval.
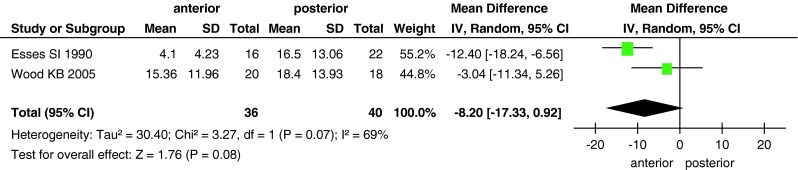
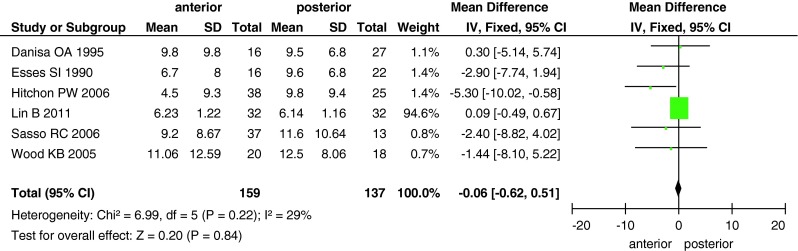
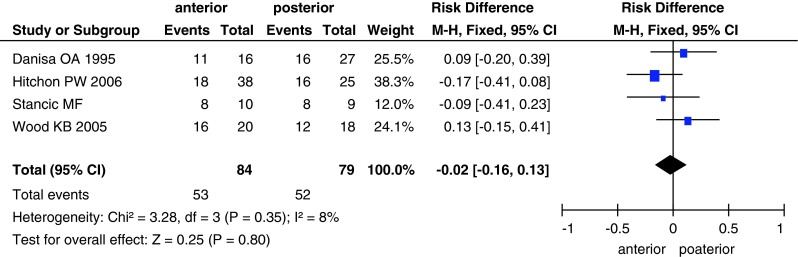
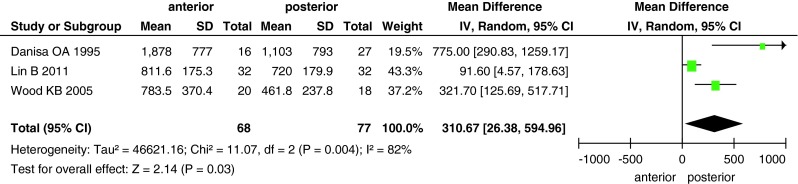
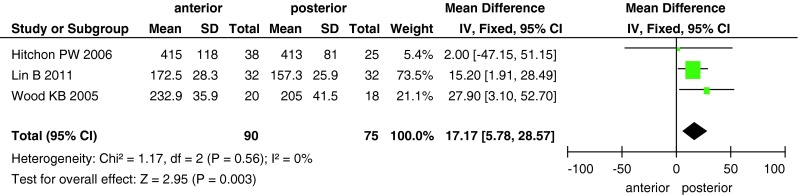
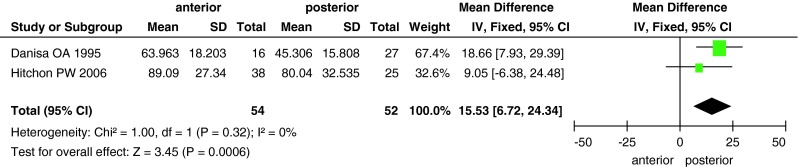
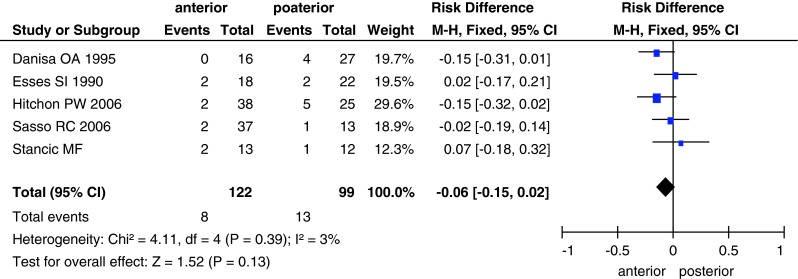
Results: Four randomized clinical trials and three controlled clinical trials comparing the results of the anterior versus posterior approach in the treatment of thoracolumbar burst fractures were retrieved; these studies included 179 and 152 patients in the anterior and posterior approach groups, respectively. There were no differences in terms of neurological recovery, return to work, complications and Cobb angle between the two groups. The anterior approach was associated with longer operative time, greater blood loss and higher cost than the posterior approach.
Conclusions: The posterior approach may be more effective than the anterior approach. However, more high-quality, randomized controlled trials are required to compare these approaches and guide clinical decision-making. Level of Evidence Level II, therapeutic study. See the Guidelines for Authors for a complete description of level of evidence.
Figures

Comment in
-
Letter regarding article by Xu et al.: anterior versus posterior approach for treatment of thoracolumbar burst fractures: a meta-analysis.Eur Spine J. 2014 Apr;23(4):940. doi: 10.1007/s00586-014-3175-4. Epub 2014 Jan 24. Eur Spine J. 2014. PMID: 24458933 Free PMC article. No abstract available.
-
Answer to the letter to the editor of Hong-Bin Guo et al. entitled "Anterior versus posterior approach for treatment of thoracolumbar burst fractures: a meta-analysis" by Gui Jun Xu, Zhi Jun Li, Jian Xiong Ma, Tao Zhang, Xin Fu, Xin Long Ma (2013); Eur Spine J (2013) 22:2176-2183.Eur Spine J. 2014 Apr;23(4):941-2. doi: 10.1007/s00586-014-3182-5. Epub 2014 Feb 19. Eur Spine J. 2014. PMID: 24549383 Free PMC article. No abstract available.
References
-
- Muller U, Berlemann U, Sledge J, Schwarzenbach O. Treatment of thoracolumbar burst fractures without neurologic deficit by indirect reduction and posterior instrumentation: bisegmental stabilization with monosegmental fusion. Eur Spine J. 1999;8(4):284–289. doi: 10.1007/s005860050175. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
