

Ipsilateral proximal femur and shaft fractures treated with hip screws and a reamed retrograde intramedullary nail
- PMID: 24014269
- PMCID: PMC4117883
- DOI: 10.1007/s11999-013-3271-5
Ipsilateral proximal femur and shaft fractures treated with hip screws and a reamed retrograde intramedullary nail
Abstract
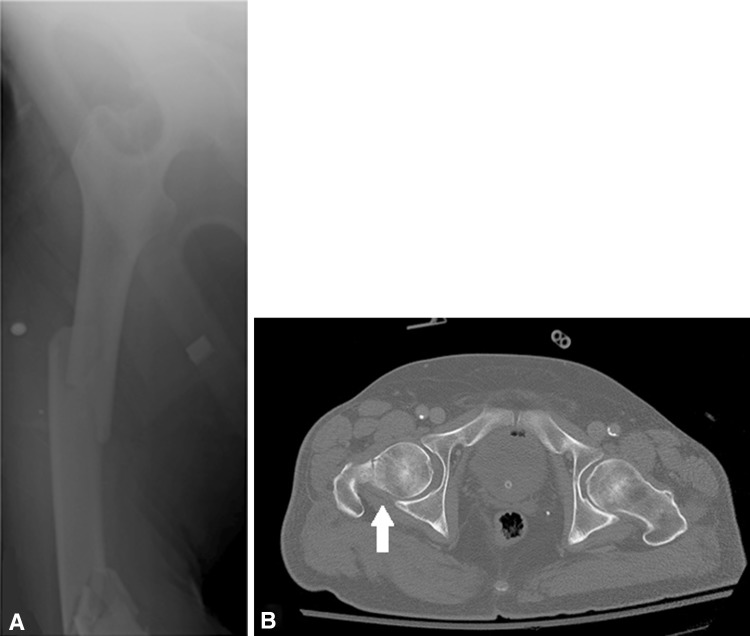
Background: Although not common, proximal femoral fractures associated with ipsilateral shaft fractures present a difficult management problem. A variety of surgical options have been employed with varying results.
Questions/purposes: We investigated the use of hip screws and a reamed retrograde intramedullary (IM) nail for the treatment of this combined fracture pattern in terms of postoperative alignment (malunion), nonunion, and complications.
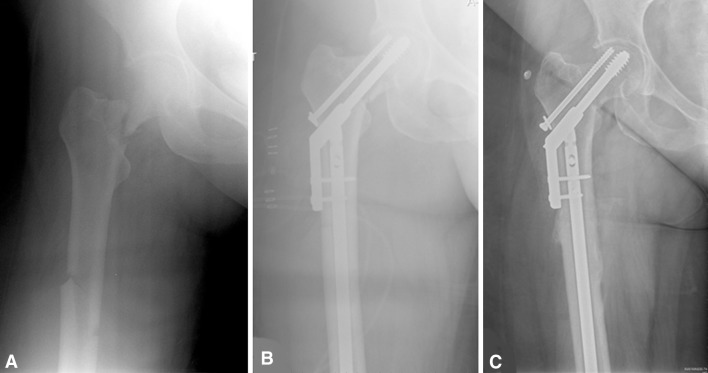
Methods: Between May 2002 and October 2011, a total of 95 proximal femoral fractures with associated shaft fractures were treated at three participating Level 1 trauma centers; all were treated with hip screw fixation (cannulated screws or sliding hip screws) and retrograde reamed IM nails. The medical records of these patients were reviewed retrospectively for alignment, malunion, nonunion, and complications. Followup was available on 92 of 95 (97%) of the patients treated with hip screws and a retrograde nail. Forty were treated with a sliding hip screw, and 52 were treated with cannulated screws.
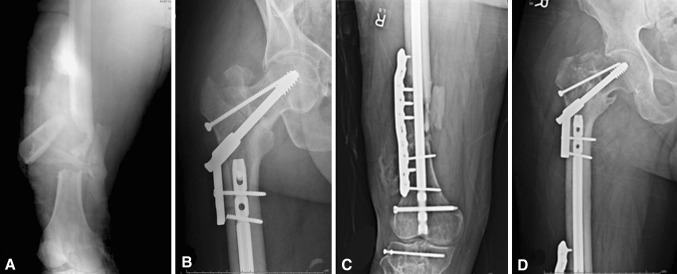
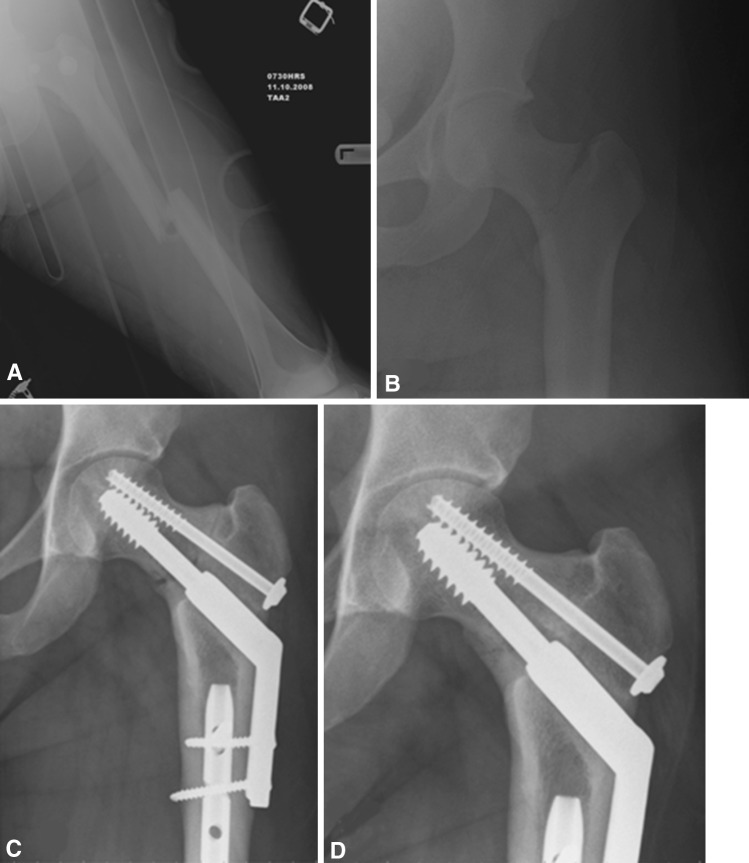
Results: There were five proximal malunions in this series (5%). The union rate was 98% (90 of 92) for the femoral neck fractures and 91.3% (84 of 92) for the femoral shaft fractures after the initial surgery. There were two nonunions of comminuted femoral neck fractures after cannulated screw fixation. There was no difference in femoral neck union or alignment when comparing cannulated screws to a sliding hip screw. Four open comminuted femoral shaft fractures went on to nonunion and required secondary surgery to obtain union, and one patient developed symptomatic avascular necrosis.
Conclusions: The treatment of ipsilateral proximal femoral neck and shaft fractures with hip screw fixation and a reamed retrograde nail demonstrated a high likelihood of union for the femoral neck fractures and a low risk of malunion. Comminution and initial displacement of the proximal femoral fracture may still lead to a small incidence of malunion or nonunion, and open comminuted femoral shaft fractures still may progress to nonunion despite appropriate surgical management.
Level of evidence: Level IV, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Figures
References
-
- Alho A. Concurrent ipsilateral fractures of the hip and shaft of the femur: a systematic review of 722 cases. Ann Chir Gynaecol. 1997;86:326–336. - PubMed
-
- Bali K, Gahlot N, Aggarwal S, Goni V. Cephalomedullary fixation for femoral neck/intertrochanteric and ipsilateral shaft fractures: surgical tips and pitfalls. Chin J Traumatol. 2013;16:40–45. - PubMed
-
- Bennett FS, Zinar DM, Kilgus DJ. Ipsilateral hip and femoral shaft fractures. Clin Orthop Relat Res. 1993;296:168–177. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
