

Outpatient endoscopic retrograde cholangiopancreatography: Safety and efficacy of anesthetic management with a natural airway in 653 consecutive procedures
- PMID: 24015127
- PMCID: PMC3757797
- DOI: 10.4103/1658-354X.115334
Outpatient endoscopic retrograde cholangiopancreatography: Safety and efficacy of anesthetic management with a natural airway in 653 consecutive procedures
Abstract
Background: Endoscopic retrograde cholangiopancreatography (ERCP) is a unique diagnostic and therapeutic procedure performed in high risk patients in prone/semi-prone position. Propofol based deep sedation has emerged as the method of choice however, the ability to predict possible complications is yet un-explored.
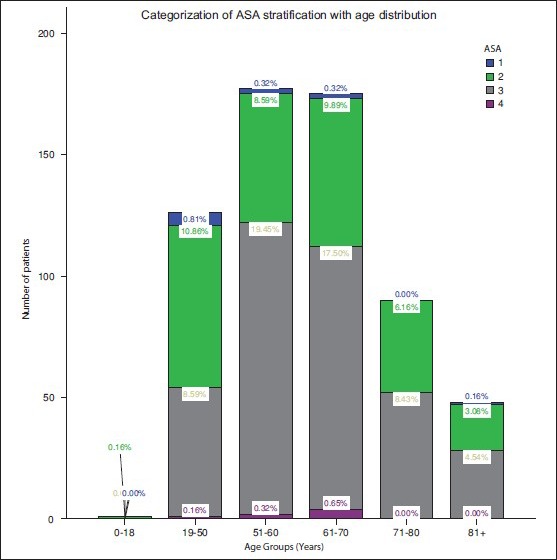
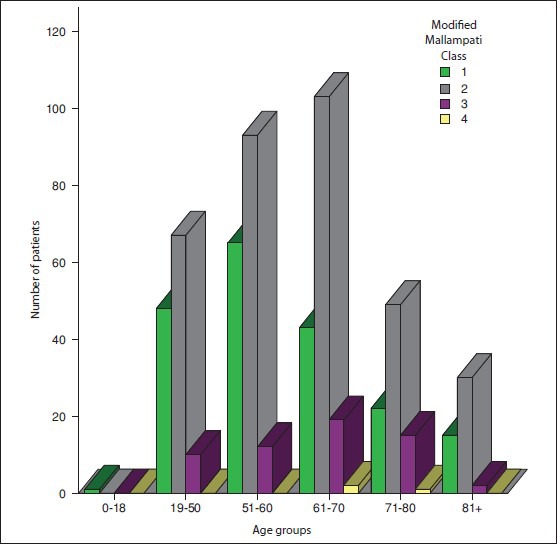
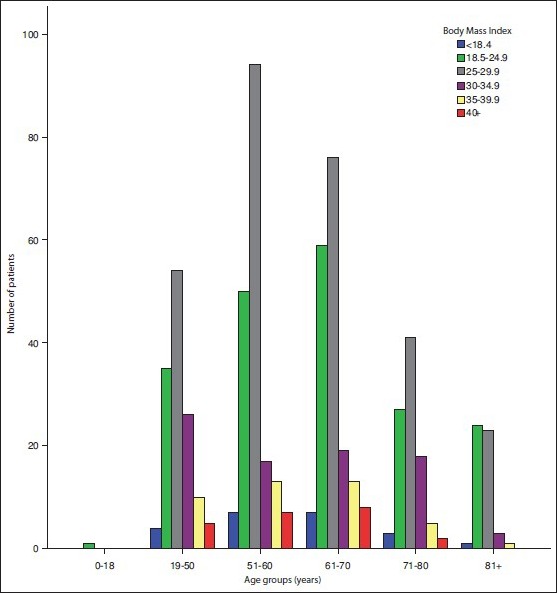
Aims: The present study aimed to evaluate known high risk-factors for general anesthesia (American Society of Anesthesiologists (ASA) status, body mass index (BMI), and Mallampati class) for their ability to affect outcomes in ERCP patients.
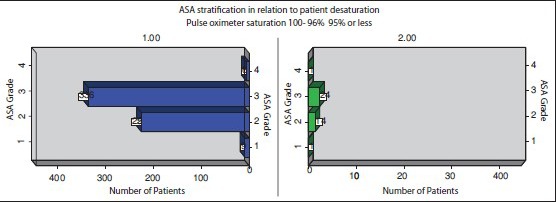
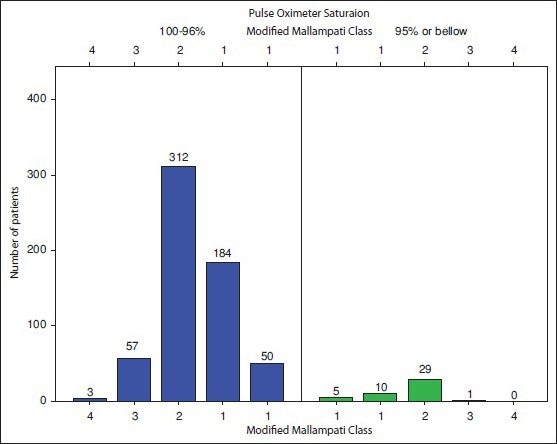
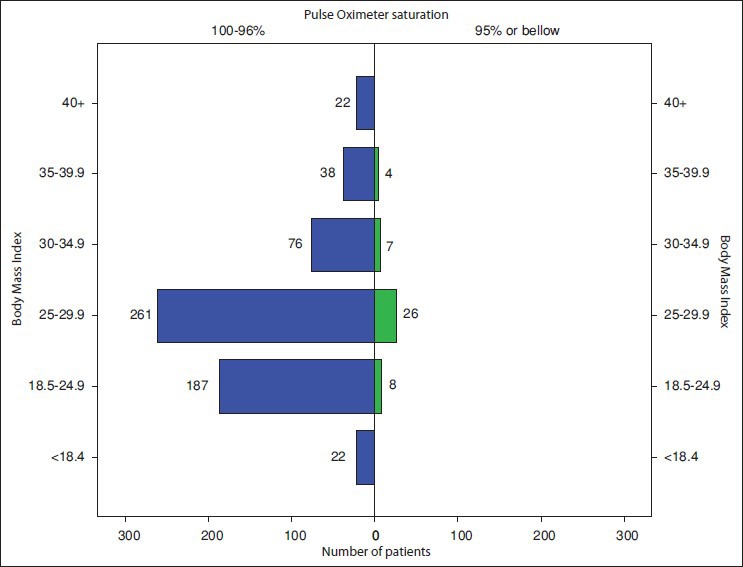
Study design: Retrospective data of 653 patients who underwent ERCP during a period of 26 months at university hospital of Pennsylvania was reviewed. Patient-specific and procedure specific data was extracted. Desaturation was defined by fall of pulse oximeter saturation below 95% and its relation to patient specific high risk-factors was analyzed.
Results: Only 45 patients had transient de-saturation below 95% without any residual sequlae. No statistically significant relation between desaturation episodes and patients higher ASA status or BMI or modified Mallampati (MMP) class was found. Despite 60% patients being ASA III/IV none required emergency intubation or procedural interruption. Optimal oxygenation and airway patency was maintained with high degree of success using simple airway maneuvers or conduit devices (nasal/oral trumpet) with oxygen supplementation in all patients.
Conclusions: Unlike general anesthesia, pre-operative patient ASA status, higher MMP or increasing BMI does not bear relation with likelihood of patients desaturating during ERCP. In presence of vigilant apnea monitoring and careful dose titration of maintenance anesthetics with airway conduits, general anesthesia, emergency intubations, and procedure interruptions can be avoided.
Keywords: Airway in endoscopic retrograde cholangiopancreatography; endoscopic retrograde cholangiopancreatography anesthesia; endoscopic retrograde cholangiopancreatography desaturation; risk predictors endoscopic retrograde cholangiopancreatography.
Conflict of interest statement
Figures

References
-
- Berzin TM, Sanaka S, Barnett SR, Sundar E, Sepe PS, Jakubowski M, et al. A prospective assessment of sedation-related adverse events and patient and endoscopist satisfaction in ERCP with anesthesiologist-administered sedation. Gastrointest Endosc. 2011;73:710–7. - PubMed
-
- American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non Anesthesiologists. Practice guidelines for sedation and analgesia by non anesthesiologists. Anesthesiology. 2002;96:1004–17. - PubMed
-
- Krugliak P, Ziff B, Rusabrov Y, Rosenthal A, Fich A, Gurman GM. Propofol versus midazolam for conscious sedation guided by processed EEG during endoscopic retrograde cholangiopancreatography: A prospective, randomized, double-blind study. Endoscopy. 2000;32:677–82. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
