

Quantification of vertebral involvement in metastatic spinal disease
- PMID: 24015159
- PMCID: PMC3763689
- DOI: 10.2174/1874325001307010286
Quantification of vertebral involvement in metastatic spinal disease
Abstract
Introduction: For patients with a solitary and well-delimitated spinal metastasis that resides inside the vertebral body, without vertebral canal invasion, and who are in good general health with a long life expectancy, en bloc spondylectomy/total vertebrectomy combined with the use of primary stabilizing instrumentation has been advocated. However, clinical experience suggests that these qualifying conditions occur very rarely.
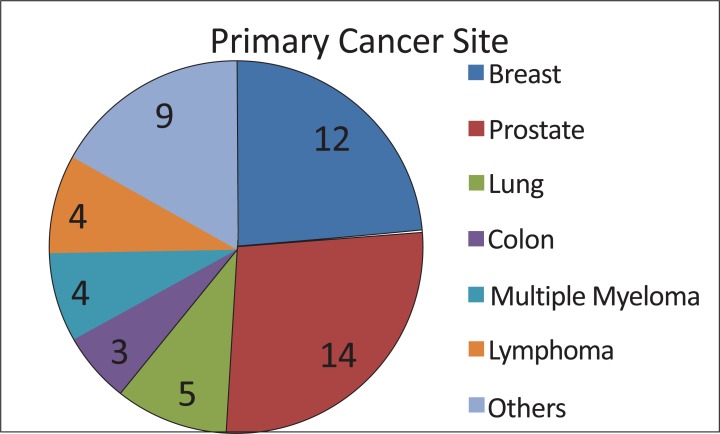
Objective: The purpose of this paper is to quantify the distribution of vertebral involvement in spinal metastases and determine the frequency with which patients can be considered candidates for radical surgery (en bloc spondylectomy).
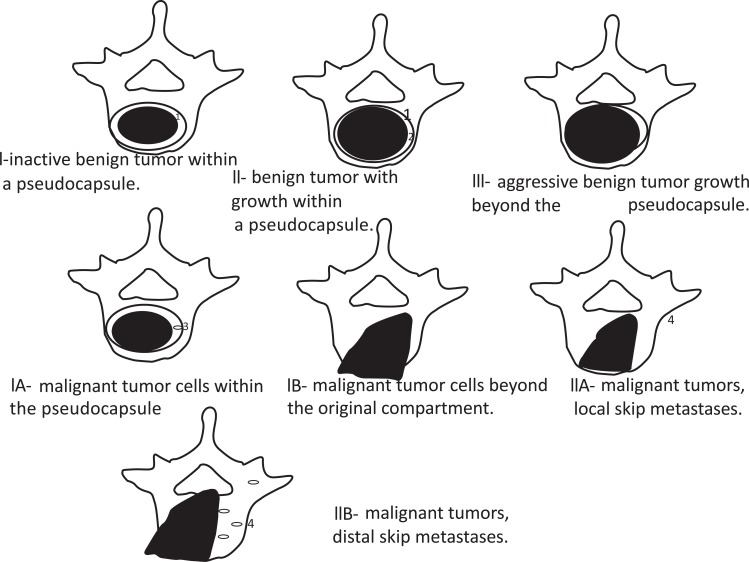
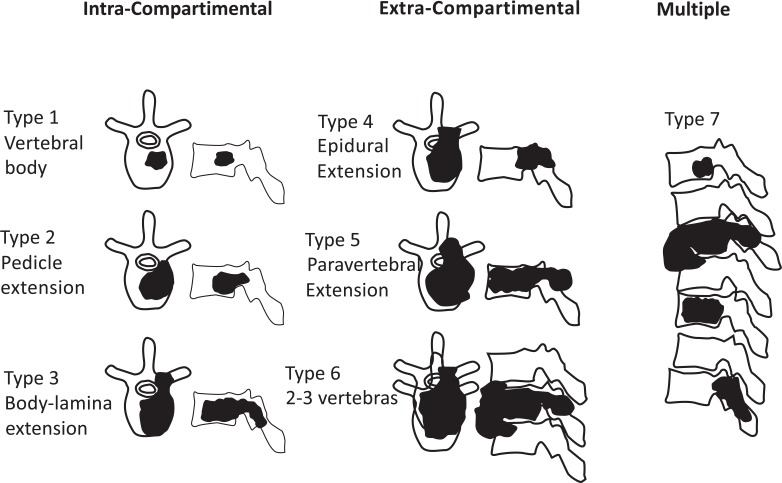
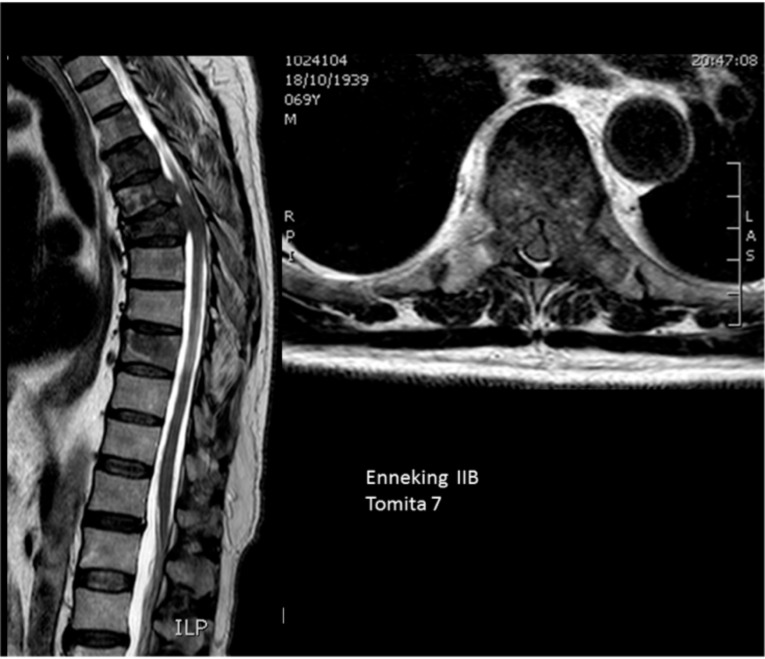
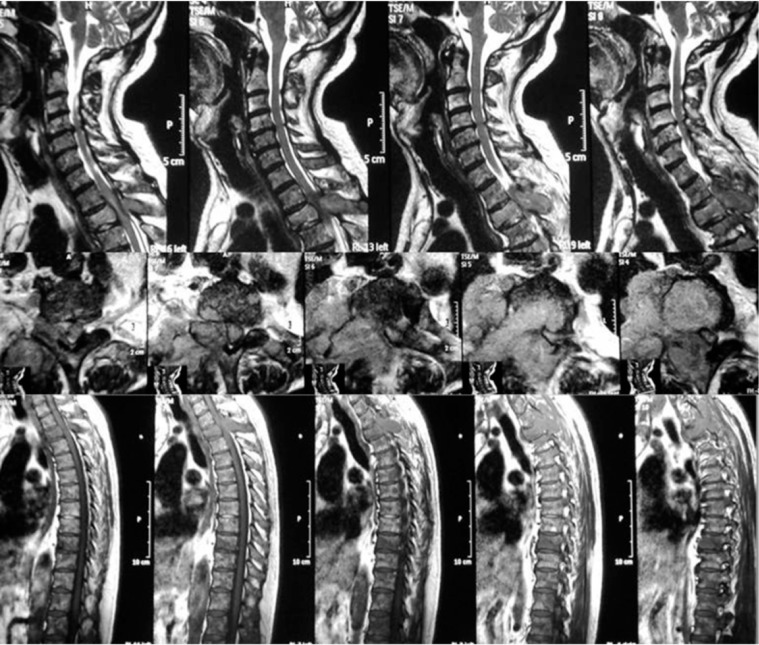
Methods: Consecutive patients were classified accordingly to Enneking's and Tomita's schemes for grading vertebral involvement of metastases.
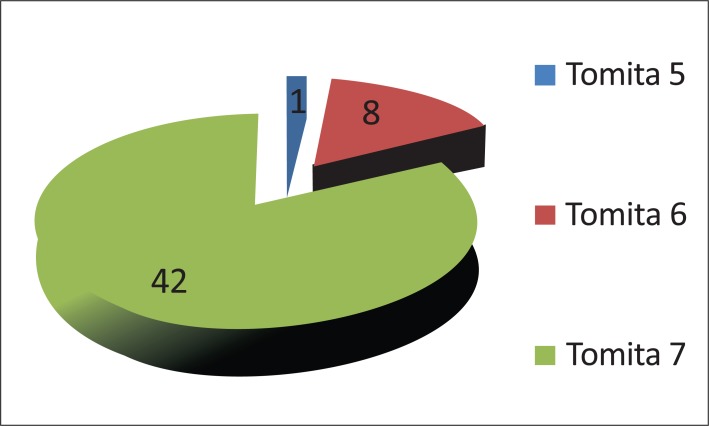
Results: Fifty-one (51) consecutive patients were evaluated. Eighty-three percent of patients presented with the involvement of multiple vertebral levels and/or spinal canal invasion.
Conclusion: Because of diffuse vertebral involvement of metastases, no patients in this sample were considered to be candidates for radical spondylectomy of vertebral metastasis.
Keywords: Cancer; neoplasm metastasis; prognosis; spine; spondylectomy; surgical procedures..
Figures
References
-
- Akbar M, Ayache A, Eichler M, Klotz M, Wiedenhöfer B, Lehner B. Management of spinal metastases, strategies and surgical indications. Orthopade. 2012;41(8):632–9. - PubMed
-
- Shiue K, Sahgal A, Chow E, et al. Management of metastatic spinal cord compression. Expert Rev Anticancer Ther. 2010;10(5):697–708. - PubMed
-
- Paton GR, Frangou E, Fourney DR. Contemporary treatment strategy for spinal metastasis: the "LMNOP" system. Can J Neurol Sci. 2011;38(3):396–403. - PubMed
-
- Kilbride L, Cox M, Kennedy CM, Lee SH, Grant R. Metastatic spinal cord compression: a review of practice and care. J Clin Nurs. 2010;19(13-14):1767–83. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials