

Provider recognition and response to echocardiographic findings indicating pulmonary hypertension in the Veterans affairs medical center population
- PMID: 24015340
- PMCID: PMC3757834
- DOI: 10.4103/2045-8932.113184
Provider recognition and response to echocardiographic findings indicating pulmonary hypertension in the Veterans affairs medical center population
Abstract
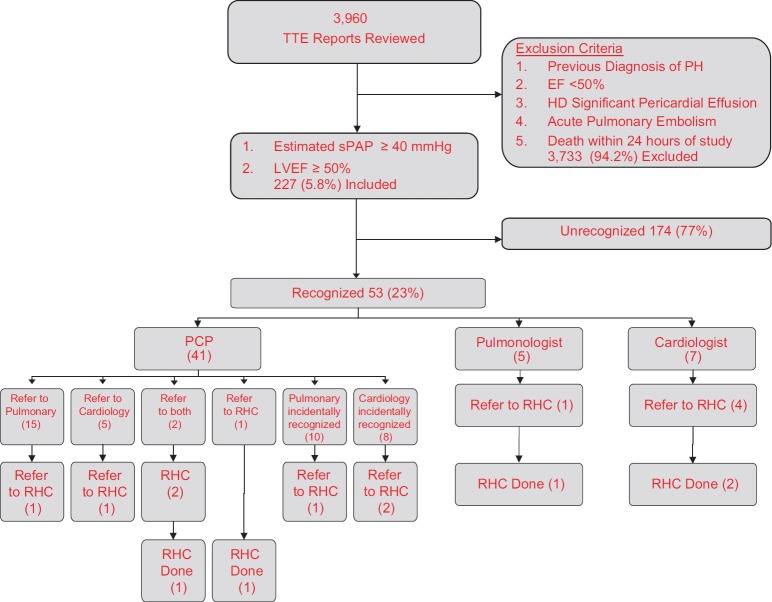
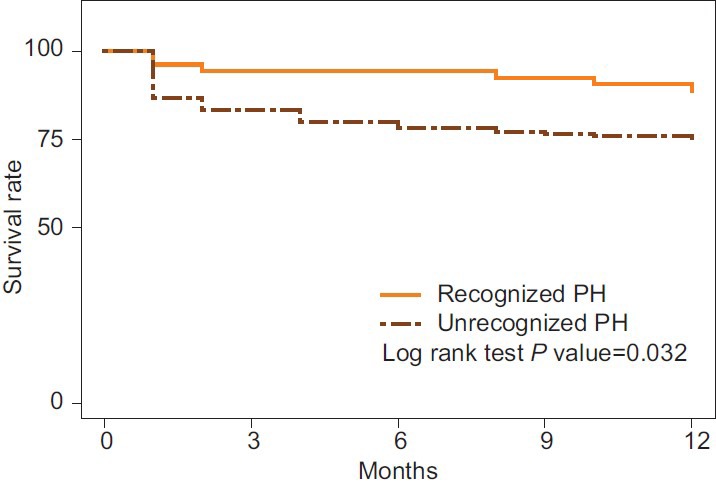
PH occurs alone or in association with many disorders. Many patients with transthoracic echocardiography (TTE) findings suggesting PH never receive additional evaluation. Patient characteristics and echocardiographic data associated with increased recognition of PH have not been fully evaluated. We evaluated TTE reports at the Cincinnati Veterans Affairs Medical Center from 2005 to 2006 retrospectively for findings highly indicative of PH: Estimated systolic pulmonary artery pressure (sPAP) ≥40 mmHg, increased right atrial or right ventricular (RV) size, or reduced RV function. Only patients with left ventricular ejection fraction (LVEF) ≥50% and no known diagnosis of PH were included. Patient characteristics, TTE findings, provider recognition rates, and subsequent referral for additional evaluation were assessed. A total of 227 of 3,960 (5.7%) TTE reports revealed findings indicating possible PH. Providers acknowledged possible PH in 53 (23.4%) reports. Recognized PH was predicted by increased RV size (odds ratio (OR) = 5.07, P < 0.001), increased right atrial dimension (OR = 6.45, P < 0.001), decreased RV function (OR = 8.86, P < 0.001), and increased PAP (OR = 1.04 corresponding to each unit increase of PAP, P < 0.01). Patients with comorbid obstructive sleep apnea (OSA), interstitial lung disease, and dyspnea were also more likely to be recognized (OR = 3.63, P = 0.021; OR = 10.98, P = 0.004; OR = 2.39, P = 0.007, respectively). The 12-month mortality rate for recognized patients, 11.3% (7/53), was lower than for unrecognized patients, 25.3% (44/174; P = 0.03). Providers recognized less than one in four patients with echocardiographic evidence suggesting PH. Echocardiography reports revealing higher PAP and right heart dilation and dysfunction are associated with increased acknowledgement of possible PH.
Keywords: disease recognition; echocardiography; pulmonary hypertension.
Conflict of interest statement
Figures
References
-
- D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–9. - PubMed
-
- Runo JR, Loyd JE. Primary pulmonary hypertension. Lancet. 2003;361:1533–44. - PubMed
-
- McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: A report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: Developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation. 2009;119:2250–94. - PubMed
-
- McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: The impact of epoprostenol therapy. Circulation. 2002;106:1477–82. - PubMed
-
- Provencher S, Jais X, Yaici A, Sitbon O, Humbert M, Simonneau G. Clinical challenges in pulmonary hypertension: Roger S. Mitchell lecture. Chest. 2005;128:622–8S. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
