

Posterior laryngitis: a disease with different aetiologies affecting health-related quality of life: a prospective case-control study
- PMID: 24015952
- PMCID: PMC3846677
- DOI: 10.1186/1472-6815-13-11
Posterior laryngitis: a disease with different aetiologies affecting health-related quality of life: a prospective case-control study
Abstract
Background: Laryngo-pharyngeal reflux (LPR) is assumed to be the most common cause of posterior laryngitis (PL). Since LPR is found in healthy subjects, and PL patients are not improved by acid-reducing therapy, other aetiologies to PL must be considered. The aims of this study in PL were to investigate the prevalence of acid reflux in the proximal oesophagus and functional gastrointestinal symptoms, to analyse motilin levels in plasma, and to assess health-related quality of life (HRQOL) before and after treatment.
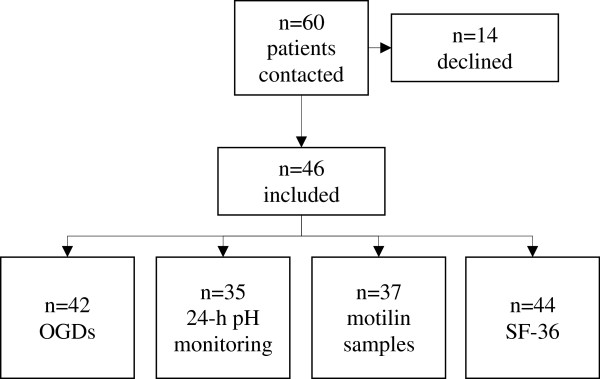
Methods: Forty-six patients (26 women), with verified PL, median age 55 (IQR 41-68) years, were referred to oesophago-gastro-duodenoscopy and 24-h pH monitoring. Plasma motilin was analysed. The 36-item Short-Form questionnaire was completed at inclusion and at follow-up after 43±14 months, when also the Visual Analogue Scale for Irritable Bowel Syndrome was completed. Values were compared to controls. Treatment and relief of symptoms were noted from medical records.
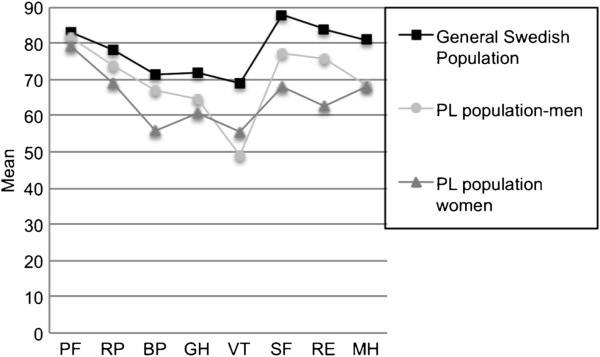
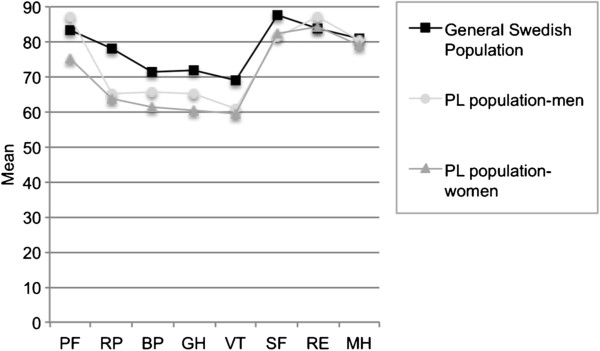
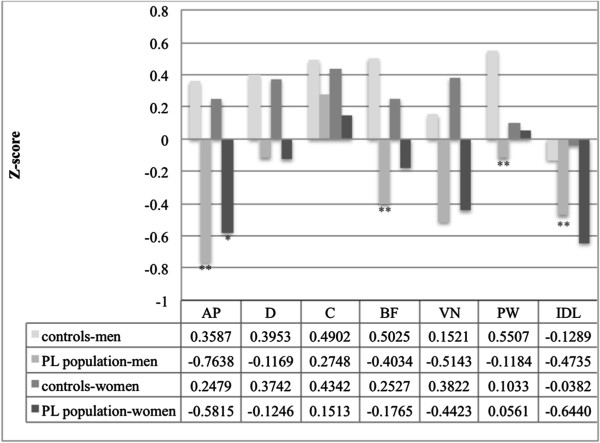
Results: Thirty-four percent had proximal acid reflux and 40% showed signs of distal reflux. Ninety-four percent received acid-reducing treatment, with total relief of symptoms in 17%. Patients with reflux symptoms had lower plasma motilin levels compared to patients without reflux symptoms (p = 0.021). The HRQOL was impaired at inclusion, but improved over time. Patients, especially men, had more functional gastrointestinal symptoms than controls.
Conclusions: This study indicates that a minority of patients with PL has LPR and is cured by acid-reducing therapy. Disturbed plasma motilin levels and presence of functional gastrointestinal symptoms are found in PL. The impaired HRQOL improves over time.
Figures
References
-
- Hopkins C, Yousaf U, Pedersen M. Acid reflux treatment for hoarsness. Cochrane Database Syst Rev. 2006;25(1):CD005054. - PubMed
-
- Pearson JP, Parikh S, Orlando RC, Johnston N, Allen J, Tinling SP, Belafsky P, Arevalo LF, Sharma N, Castell DO. et al. Review article: reflux and its consequences--the laryngeal, pulmonary and oesophageal manifestations. Conference held in conjunction with the 9th International Symposium on Human Pepsin (ISHP) Kingston-upon-Hull, UK, 21–23 April 2010. Aliment Pharm Ther. 2011;33(Suppl 1):1–71. - PubMed
-
- Watson MG. Review article:laryngopharyngeal reflux-the ear, nose and throat patient. Aliment Pharm Ther. 2011;33(Suppl 1):53–57.
LinkOut - more resources
Full Text Sources
Other Literature Sources
