

The relation of weight suppression and body mass index to symptomatology and treatment response in anorexia nervosa
- PMID: 24016010
- PMCID: PMC4096540
- DOI: 10.1037/a0033930
The relation of weight suppression and body mass index to symptomatology and treatment response in anorexia nervosa
Abstract
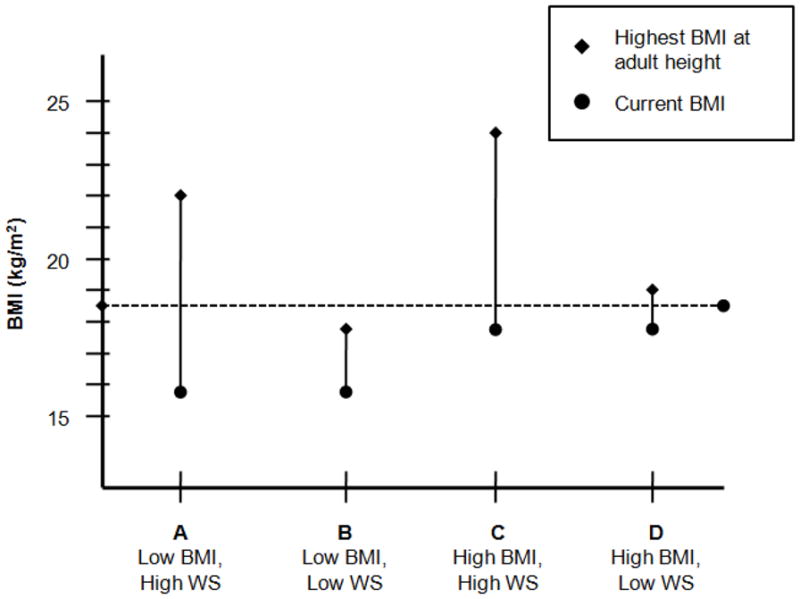
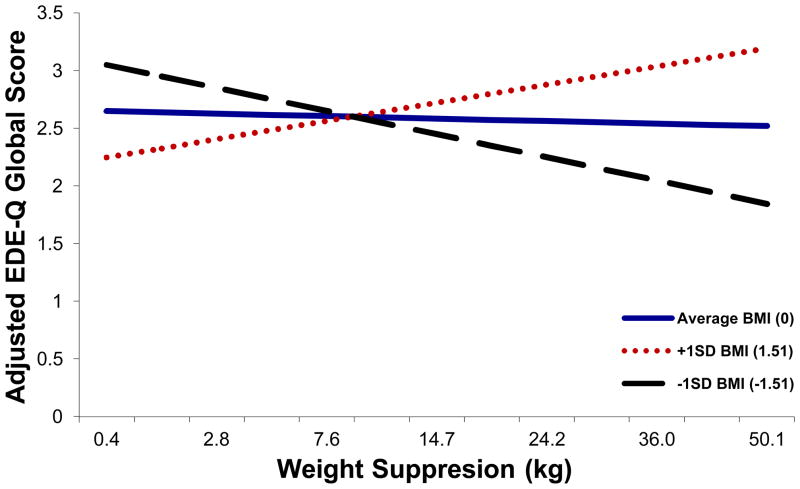
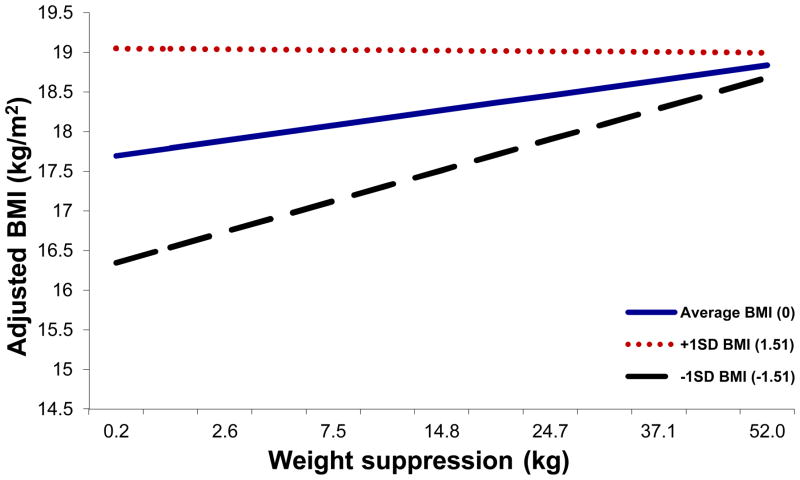
Weight suppression, the difference between highest past weight and current weight, is a robust predictor of clinical characteristics of bulimia nervosa; however, the influence of weight suppression in anorexia nervosa (AN) has been little studied, and to our knowledge, no study to date has investigated the ways in which the relevance of weight suppression in AN may depend upon an individual's current body mass index (BMI). The present study investigated weight suppression, BMI, and their interaction as cross-sectional and prospective predictors of psychological symptoms and weight in AN. Women with AN completed depression (Beck Depression Inventory-II) and eating disorder symptomatology measures (Eating Disorder Examination Questionnaire and Eating Disorders Inventory-3) at residential treatment admission (N = 350) and discharge (N = 238). Weight suppression and BMI were weakly correlated (r = -.22). At admission, BMI was positively correlated with all symptom measures except Restraint and Depression scores. Weight suppression was also independently positively correlated with all measures except Weight Concern and Body Dissatisfaction subscale scores. In analyses examining discharge scores (including admission values as covariates), the admission weight suppression × BMI interaction consistently predicted posttreatment psychopathology. Controlling for weight gain in treatment and age, higher admission weight suppression predicted lower discharge scores (less symptom endorsement) among those with lower BMIs; among those with higher BMIs, higher weight suppression predicted higher discharge scores. These results are the first to our knowledge to demonstrate that absolute and relative weight status are joint indicators of AN severity and prognosis. These findings may have major implications for conceptualization and treatment of AN.
PsycINFO Database Record (c) 2013 APA, all rights reserved.
Figures
References
-
- American Psychiatric Association. Practice guideline for eating disorders. American Journal of Psychiatry. 1993;150:208–228. - PubMed
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Fouth Edition (DSM-IV) Washington, D.C: American Psychiatric Association; 1994.
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Fouth Edition, Text Revision (DSM-IV-TR) Washington, DC: American Psychiatric Association; 2000.
-
- American Psychiatric Association. Practice Guideline for the Treatment of Patients With Eating Disorders. 3. Washington, D.C: American Psychiatric Association (APA); 2006.
-
- American Psychiatric Association. DSM-5 Development. 2012;2012 from http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=26.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
