

Infrequent dialysis: a new paradigm for hemodialysis initiation
- PMID: 24016197
- PMCID: PMC3844666
- DOI: 10.1111/sdi.12133
Infrequent dialysis: a new paradigm for hemodialysis initiation
Abstract
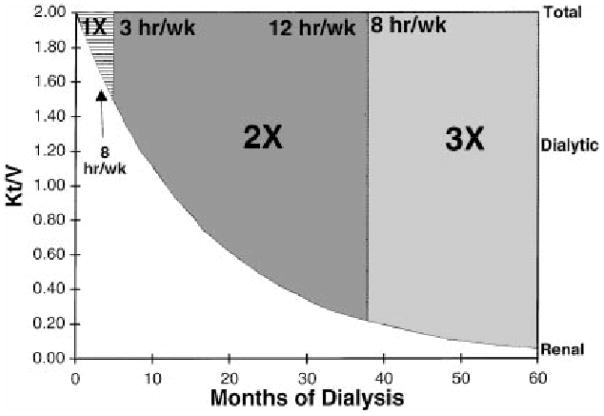
Nearly a half-century ago, the thrice-weekly hemodialysis schedule was empirically established as a means to provide an adequate dialysis dose while also treating the greatest number of end-stage renal disease (ESRD) patients using limited resources. Landmark trials of hemodialysis adequacy have historically been anchored to thrice-weekly regimens, but a recent randomized controlled trial demonstrated that frequent hemodialysis (six times per week) confers cardiovascular and survival benefits. Based on these collective data and experience, clinical practice guidelines advise against a less than thrice-weekly treatment schedule in patients without residual renal function, yet provide limited guidance on the optimal treatment frequency when substantial native kidney function is present. Thus, during the transition from Stage 5 chronic kidney disease to ESRD, the current paradigm is to initiate hemodialysis on a "full-dose" thrice-weekly regimen even among patients with substantial residual renal function. However, emerging data suggest that frequent hemodialysis accelerates residual renal function decline, and infrequent regimens may provide better preservation of native kidney function. Given the high mortality rates during the first 6 months of hemodialysis and the survival benefits of preserved native kidney function, initiation with twice-weekly treatment schedules ("infrequent hemodialysis") with an incremental increase in frequency over time may provide an opportunity to optimize patient survival. This review outlines the clinical benefits of post-hemodialysis residual renal function, studies of twice-weekly treatment regimens, and the potential risks and benefits of infrequent hemodialysis.
© 2013 Wiley Periodicals, Inc.
Figures
Comment in
-
What Is Known and Unknown About Twice-Weekly Hemodialysis.Blood Purif. 2015;40(4):298-305. doi: 10.1159/000441577. Epub 2015 Nov 17. Blood Purif. 2015. PMID: 26656764 Free PMC article.
References
-
- U.S. Renal Data System. USRDS 2012 Annual Data Report: Atlas of End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2012.
-
- NKF-DOQI clinical practice guidelines for peritoneal dialysis adequacy. National Kidney Foundation. Am J Kidney Dis. 1997;30(3 Suppl 2):S67–136. - PubMed
-
- Canaud B. Residual renal function: the delicate balance between benefits and risks. Nephrol Dial Transplant. 2008;23(6):1801–1805. - PubMed
-
- Chandna SM, Farrington K. Residual renal function: considerations on its importance and preservation in dialysis patients. Semin Dial. 2004;17(3):196–201. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
