

Re-do Roux-en-Y gastric bypass in a patient with known midgut malrotation
- PMID: 24018088
- PMCID: PMC3771770
- DOI: 10.4293/108680813x13753907291990
Re-do Roux-en-Y gastric bypass in a patient with known midgut malrotation
Abstract
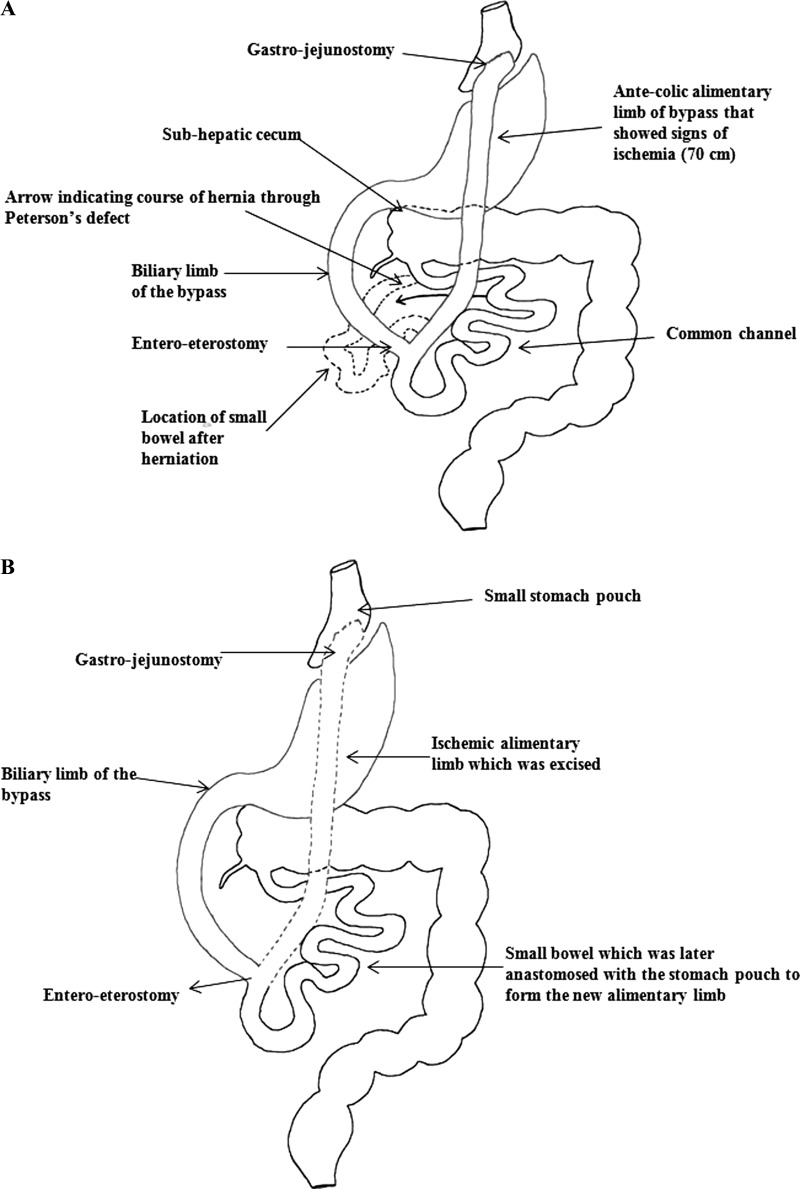
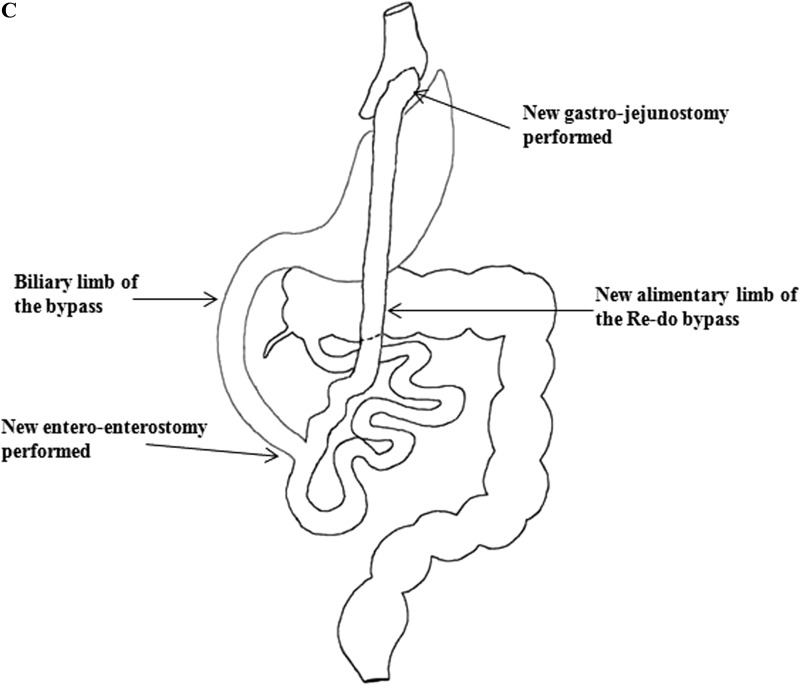
A 40-year-old woman presented with small bowel obstruction caused by an internal hernia through Peterson's defect. The patient was known to have midgut malrotation (MM) and also had laparoscopic Roux-en-Y gastric bypass for morbid obesity 6 years prior. An open revision of Roux-en-Y gastric bypass was performed as a result of ischemia of alimentary limb. She made a slow but uneventful recovery and was discharged home. MM is a rare congenital anomaly that requires the surgeon to be well aware of the unique variation in anatomy to perform a mirror image of the routine Roux-en-Y gastric bypass. At the end of this case report, we present a short literature review of published data related to MM encountered during Roux-en-Y gastric bypass.
Figures


References
-
- Pickhardt PJ, Bhalla S. Intestinal malrotation in adolescents and adults: spectrum of clinical and imaging features. Am J Roentgenol. 2002;179:1429–1435 - PubMed
-
- Shew SB. Surgical concerns in malrotation and midgut volvulus. Pediatr Radiol. 2009;39 Suppl 2:S167–S171 - PubMed
-
- Langman J. Digestive system. In: Sadler TW, ed. Langman's Medical Embryology. Ninth ed Montana: Lippincott Williams & Wilkins; 2003:285–320
-
- Alami RS, Schuster R, Morton JM, et al. Robotic-assisted laparoscopic Roux-en-Y gastric bypass in a patient with midgut Malrotation. Surg Obes Relat Dis. 2006;2:222–225 - PubMed
-
- Palepu RP, Harmon CM, Goldberg SP, et al. Intestinal malrotation discovered at the time of laparoscopic roux-en-Y gastric bypass. J Gastrointest Surg. 2007;11:898–902 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials