

Evaluation of bone marrow lesion volume as a knee osteoarthritis biomarker--longitudinal relationships with pain and structural changes: data from the Osteoarthritis Initiative
- PMID: 24020939
- PMCID: PMC3978948
- DOI: 10.1186/ar4292
Evaluation of bone marrow lesion volume as a knee osteoarthritis biomarker--longitudinal relationships with pain and structural changes: data from the Osteoarthritis Initiative
Abstract
Introduction: Bone marrow lesion (BML) size may be an important imaging biomarker for osteoarthritis-related clinical trials and reducing BML size may be an important therapeutic goal. However, data on the interrelationships between BML size, pain, and structural progression are inconsistent and rarely examined in the same cohort. Therefore, we evaluated the cross-sectional and longitudinal associations of BML volume with knee pain and joint space narrowing (JSN).
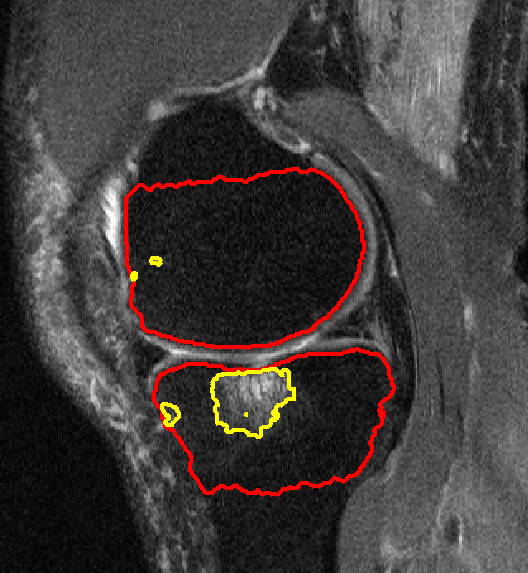
Methods: A BML volume assessment was performed on magnetic resonance images of the knee collected at the 24- and 48-month Osteoarthritis Initiative visits from a convenience sample of 404 participants in the progression cohort. During the same visits, knee pain was assessed with WOMAC pain scores and knee radiographs were acquired and scored for JSN. BML volume was summed to generate a total knee volume and an index tibiofemoral compartment volume (compartment with greater baseline JSN). Primary analyses included multiple linear regressions (outcome = pain, predictor = total knee BML volume) and logistic regressions (outcome = JSN, predictor = index tibiofemoral compartment BML volume).
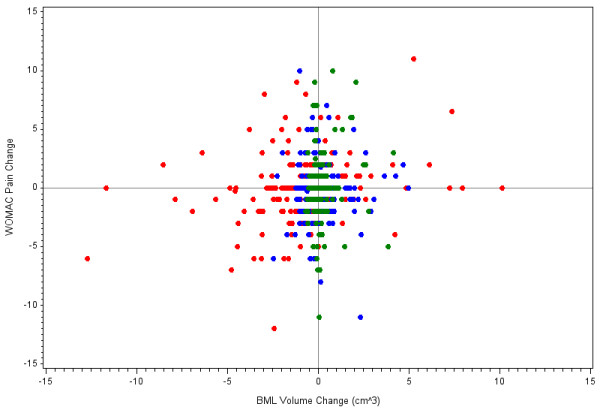
Results: This sample was 49% female with a mean age of 63 (9.2 standard deviation (SD)) years, and 71% had radiographic osteoarthritis in the study knee. Larger baseline BMLs were associated with greater baseline knee pain (P = 0.01), the presence of JSN at baseline (odds ratio (OR) = 1.50, 95% confidence interval (CI) = 1.23 to 1.83), and JSN progression (OR = 1.27, 95%CI = 1.11 to 1.46). Changes in total knee BML volume had a positive association with changes in knee pain severity (P = 0.004) and this association may be driven by knees that were progressing from no or small baseline BMLs to larger BMLs. In contrast, we found no linear positive relationship between BML volume change and JSN progression. Instead, regression of medial tibiofemoral BML volume was associated with JSN progression compared to knees with no or minimal changes in BML volume (OR = 3.36, 95%CI = 1.55 to 7.28). However, follow-up analyses indicated that the association between JSN progression and BML volume change may primarily be influenced by baseline BML volume.
Conclusion: Large baseline BMLs are associated with greater baseline knee pain, the presence of JSN at baseline, and disease progression. Additionally, BML regression is associated with decreased knee pain but not a reduced risk of concurrent JSN progression.
Figures
References
-
- Lo GH, McAlindon TE, Niu J, Zhang Y, Beals C, Dabrowski C, Le Graverand MP, Hunter DJ. Bone marrow lesions and joint effusion are strongly and independently associated with weight-bearing pain in knee osteoarthritis: data from the Osteoarthritis Initiative. Osteoarthritis Cartilage. 2009;15:1562–1569. - PMC - PubMed
-
- Tanamas SK, Wluka AE, Pelletier JP, Pelletier JM, Abram F, Berry PA, Wang Y, Jones G, Cicuttini FM. Bone marrow lesions in people with knee osteoarthritis predict progression of disease and joint replacement: a longitudinal study. Rheumatology (Oxford) 2010;15:2413–2419. - PubMed
-
- Sowers MF, Hayes C, Jamadar D, Capul D, Lachance L, Jannausch M, Welch G. Magnetic resonance-detected subchondral bone marrow and cartilage defect characteristics associated with pain and X-ray-defined knee osteoarthritis. Osteoarthritis Cartilage. 2003;15:387–393. - PubMed
-
- Yusuf E, Kortekaas MC, Watt I, Huizinga TW, Kloppenburg M. Do knee abnormalities visualised on MRI explain knee pain in knee osteoarthritis? A systematic review. Ann Rheum Dis. 2011;15:60–67. - PubMed
-
- Raynauld JP, Martel-Pelletier J, Berthiaume MJ, Abram F, Choquette D, Haraoui B, Beary JF, Cline GA, Meyer JM, Pelletier JP. Correlation between bone lesion changes and cartilage volume loss in patients with osteoarthritis of the knee as assessed by quantitative magnetic resonance imaging over a 24-month period. Ann Rheum Dis. 2008;15:683–688. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
