

Recent trends in HIV-1 drug resistance
- PMID: 24021560
- PMCID: PMC3963152
- DOI: 10.1016/j.coviro.2013.08.007
Recent trends in HIV-1 drug resistance
Abstract
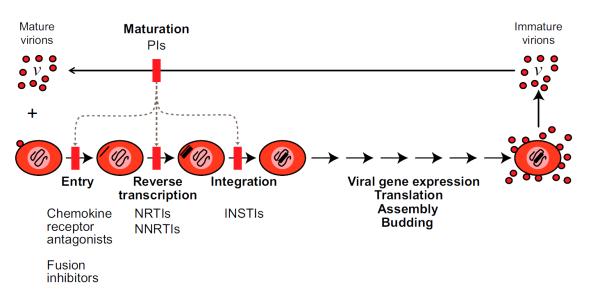
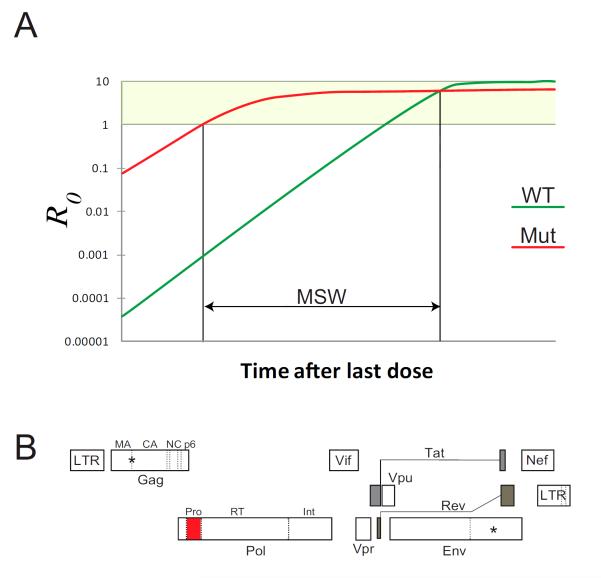
Once considered an inevitable consequence of HIV treatment, drug resistance is declining. This decline supports the hypothesis that antiretroviral therapy can arrest replication and prevent the evolution of resistance. Further support comes from excellent clinical outcomes, the failure of treatment intensification to reduce residual viremia, the lack of viral evolution in patients on optimal therapy, pharmacodynamics studies explaining the extraordinarily high antiviral activity of modern regimens, and recent reports of potential cures. Evidence supporting ongoing replication includes higher rates of certain complications in treated patients and an increase in circular forms of the viral genome after intensification with integrase inhibitors. Recent studies also provide an explanation for the observation that some patients fail protease-inhibitor based regimens without evidence for resistance.
Copyright © 2013 Elsevier B.V. All rights reserved.
Figures
References
-
- Larder BA, Darby G, Richman DD. HIV with reduced sensitivity to zidovudine (AZT) isolated during prolonged therapy. Science. 1989;243:1731–1734. - PubMed
-
- This comprehensive summary of well characterized HIV-1 drug resistance mutations is compiled and updated by a panel of experts. Because of the close correlation between genotype and phenotype for HIV-1 drug resistance, the detection of these mutations by sequence analysis provides information that is extremely useful in patient management.
-
- Gulick RM, Mellors JW, Havlir D, Eron JJ, Gonzalez C, McMahon D, Richman DD, Valentine FT, Jonas L, Meibohm A, et al. Treatment with indinavir, zidovudine, and lamivudine in adults with human immunodeficiency virus infection and prior antiretroviral therapy. N.Engl.J.Med. 1997;337:734–739. - PubMed
-
- Hammer SM, Squires KE, Hughes MD, Grimes JM, Demeter LM, Currier JS, Eron JJ, Jr, Feinberg JE, Balfour HH, Jr, Deyton LR, et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. AIDS Clinical Trials Group 320 Study Team. N.Engl.J.Med. 1997;337:725–733. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
