

Diabetes insipidus contributes to traumatic brain injury pathology via CD36 neuroinflammation
- PMID: 24021616
- PMCID: PMC3818499
- DOI: 10.1016/j.mehy.2013.08.022
Diabetes insipidus contributes to traumatic brain injury pathology via CD36 neuroinflammation
Abstract
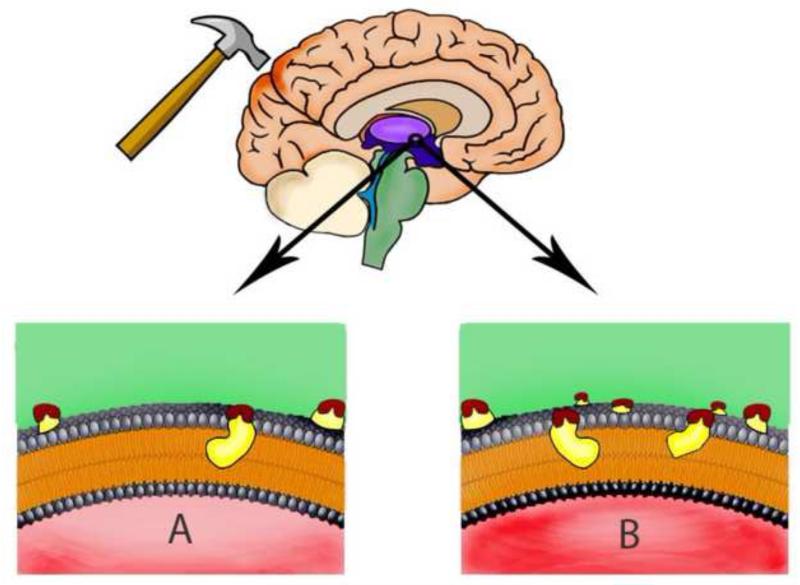
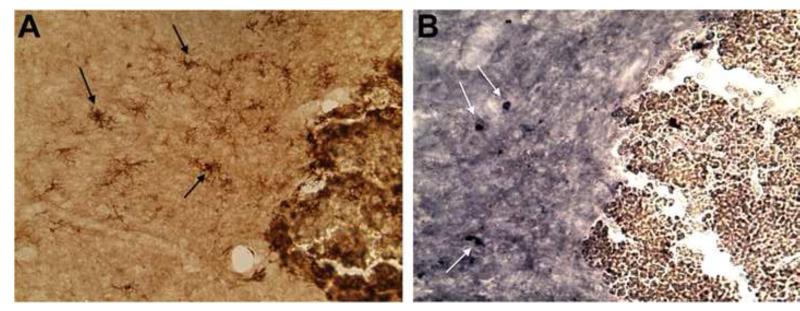
Each year, over one million people in the United States are affected by traumatic brain injury (TBI). Symptoms of both acute and chronic neuroinflammation follow TBI, coinciding with a robust immune response and activation of the brain's endogenous repair mechanisms. TBI can lead to endocrine failure as a result of damage to the thalamic region of the brain, evidenced by excessive thirst and polyuria often accompanying TBI. These symptoms indicate the presence of diabetes insipidus (DI), a disruption of water homeostasis due to antidiuretic hormone deficiency. This deficiency accompanies a mechanical or neuroinflammatory damage to the thalamic region during TBI, evidenced by increased expression of inflammatory microglial marker MHCII in this brain region. Excessive thirst and urinations, which are typical DI symptoms, in our chronic TBI rats also suggest a close connection between TBI and DI. We seek to bridge this gap between TBI and DI through investigation of the Cluster of Differentiation 36 (CD36) receptor. This receptor is associated with Low-Density Lipoprotein (LDL) deregulation, pro-inflammatory events, and innate immunity regulation. We posit that CD36 exacerbates TBI through immune activation and subsequent neuroinflammation. Indeed, scientific evidence already supports pathological interaction of CD36 in other neurological disorders including stroke and Alzheimer's disease. We propose that DI contributes to TBI pathology via CD36 neuroinflammation. Use of CD36 as a biomarker may provide insights into treatment and disease pathology of TBI and DI. This unexplored avenue of research holds potential for a better understanding and treatment of TBI and DI.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
References
-
- Faul M, Xu L, Wald MM, Coronado VG. [Accessed July 14, 2013];Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002–2006. 2010 http://www.cdc.gov/traumaticbraininjury/pdf/blue_book.pdf.
-
- Hannon MJ, Finucane FM, Sherlock M, Agha A, Thompson CJ. Disorders of water homeostasis in Neurosurgical Patients. J Clin Endocrinol Metab. 2012;97(5):1423–33. - PubMed
-
- Agha A, Sherlock M, Phillips J, Tormey W, Thompson CJ. The natural history of post-traumatic neurohypophysial dysfunction. Eur J Endocrinol. 2005;52(3):371–7. - PubMed
-
- Tsagarkis S, Tzanela M, Dimopoulou I. Diabetes insipidus, secondary hypoadenalism and hypothyroidism after traumatic brain injury: clinical implications. Pituitary. 2005;8(3-4):251–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
