

Prospective validation of the computed tomographic angiography spot sign score for intracerebral hemorrhage
- PMID: 24021687
- PMCID: PMC4187102
- DOI: 10.1161/STROKEAHA.113.002752
Prospective validation of the computed tomographic angiography spot sign score for intracerebral hemorrhage
Erratum in
- Stroke. 2013 Nov;44(11):161
Abstract
Background and purpose: Intracerebral hemorrhage (ICH) results in high mortality and morbidity for patients. Previous retrospective studies correlated the spot sign score (SSSc) with ICH expansion, mortality, and clinical outcome among ICH survivors. We performed a prospective study to validate the SSSc for the prediction of ICH expansion, mortality, and clinical outcome among survivors.
Methods: We prospectively included consecutive patients with primary ICH presenting to a single institution for a 1.5-year period. All patients underwent baseline noncontrast computed tomography (CT) and multidetector CT angiography performed within 24 hours of admission and a follow-up noncontrast CT within 48 hours after the initial CT. The ICH volume was calculated on the noncontrast CT images using semiautomated software. The SSSc was calculated on the multidetector CT angiographic source images. We assessed in-hospital mortality and modified Rankin Scale at discharge and at 3 months among survivors. A multivariate logistic regression analysis was performed to determine independent predictors of hematoma expansion, in-hospital mortality, and poor clinical outcome.
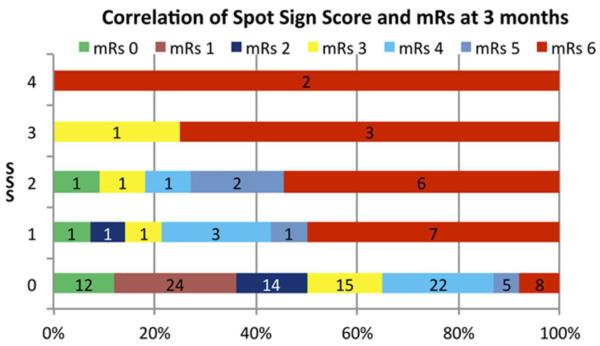
Results: A total of 131 patients met the inclusion criteria. Of the 131 patients, a spot sign was detected in 31 patients (24%). In a multivariate analysis, the SSSc predicted significant hematoma expansion (odds ratio, 3.1; 95% confidence interval, 1.77-5.39; P≤0.0001), in-hospital mortality (odds ratio, 4.1; 95% confidence interval, 2.11-7.94; P≤0.0001), and poor clinical outcome (odds ratio, 3; 95% confidence interval, 1.4-4.42; P=0.004). In addition, the SSSc was an accurate grading scale for ICH expansion, modified Rankin Scale at discharge, and in-hospital mortality.
Conclusions: The SSSc demonstrated a strong stepwise correlation with hematoma expansion and clinical outcome in patients with primary ICH.
Keywords: CT angiography; intracerebral hemorrhage; mortality; spot sign; stroke.
Figures
References
-
- Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF. Spontaneous intracerebral hemorrhage. N Engl J Med. 2001;344:1450–1460. - PubMed
-
- Zhang LF, Yang J, Hong Z, Yuan GG, Zhou BF, Zhao LC, et al. Proportion of different subtypes of stroke in china. Stroke. 2003;34:2091–2096. - PubMed
-
- Hemphill JC, 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ich score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001;32:891–897. - PubMed
-
- Leira R, Davalos A, Silva Y, Gil-Peralta A, Tejada J, Garcia M, et al. Early neurologic deterioration in intracerebral hemorrhage: Predictors and associated factors. Neurology. 2004;63:461–467. - PubMed
-
- Rost NS, Smith EE, Chang Y, Snider RW, Chanderraj R, Schwab K, et al. Prediction of functional outcome in patients with primary intracerebral hemorrhage: The func score. Stroke. 2008;39:2304–2309. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
