

Cytomegalovirus in the neonate: immune correlates of infection and protection
- PMID: 24023565
- PMCID: PMC3760263
- DOI: 10.1155/2013/501801
Cytomegalovirus in the neonate: immune correlates of infection and protection
Abstract
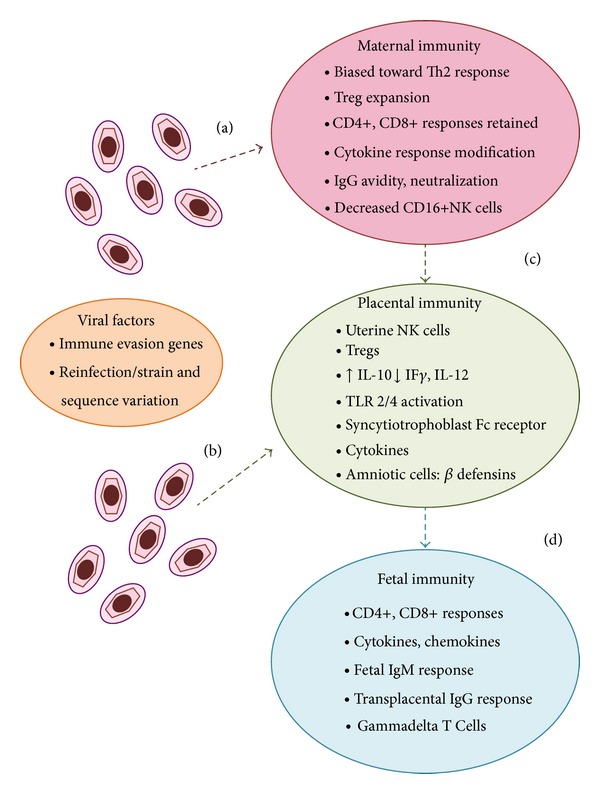
Fetal and neonatal infections caused by human cytomegalovirus (CMV) are important causes of morbidity and occasional mortality. Development of a vaccine against congenital CMV infection is a major public health priority. Vaccine design is currently focused on strategies that aim to elicit neutralizing antibody and T-cell responses, toward the goal of preventing primary or recurrent infection in women of child-bearing age. However, there has been relatively little attention given to understanding the mechanisms of immune protection against acquisition of CMV infection in the fetus and newborn and how this information might be exploited for vaccine design. There has similarly been an insufficient study of what deficits in the immune response to CMV, both for mother and fetus, may increase susceptibility to congenital infection and disease. Protection of the fetus against vertical transmission can likely be achieved by protection of the placenta, which has its own unique immunological milieu, further complicating the analysis of the correlates of protective immunity. In this review, the current state of knowledge about immune effectors of protection against CMV in the maternal, placental, and fetal compartments is reviewed. A better understanding of immune responses that prevent and/or predispose to infection will help in the development of novel vaccine strategies.
Figures
References
-
- Kenneson A, Cannon MJ. Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Reviews in Medical Virology. 2007;17(4):253–276. - PubMed
-
- Wang C, Zhang X, Bialek S, Cannon MJ. Attribution of congenital cytomegalovirus infection to primary versus non-primary maternal infection. Clinical Infectious Diseases. 2011;52(2):e11–e13. - PubMed
-
- Whitley RJ. Congenital cytomegalovirus infection: epidemiology and treatment. Advances in Experimental Medicine and Biology. 2004;549:155–160. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
