

Imaging appearance of treated hepatocellular carcinoma
- PMID: 24023980
- PMCID: PMC3767840
- DOI: 10.4254/wjh.v5.i8.417
Imaging appearance of treated hepatocellular carcinoma
Abstract
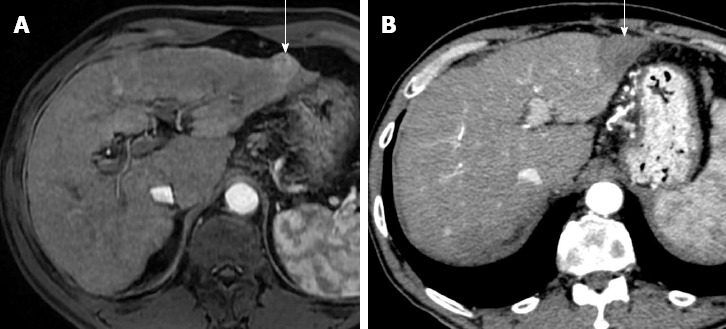
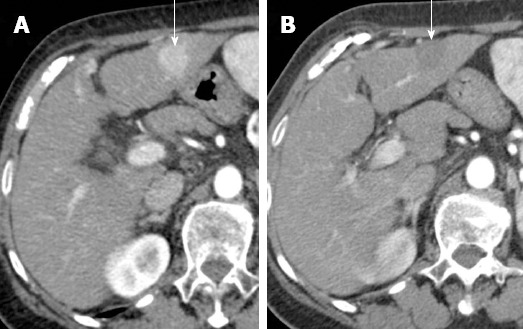
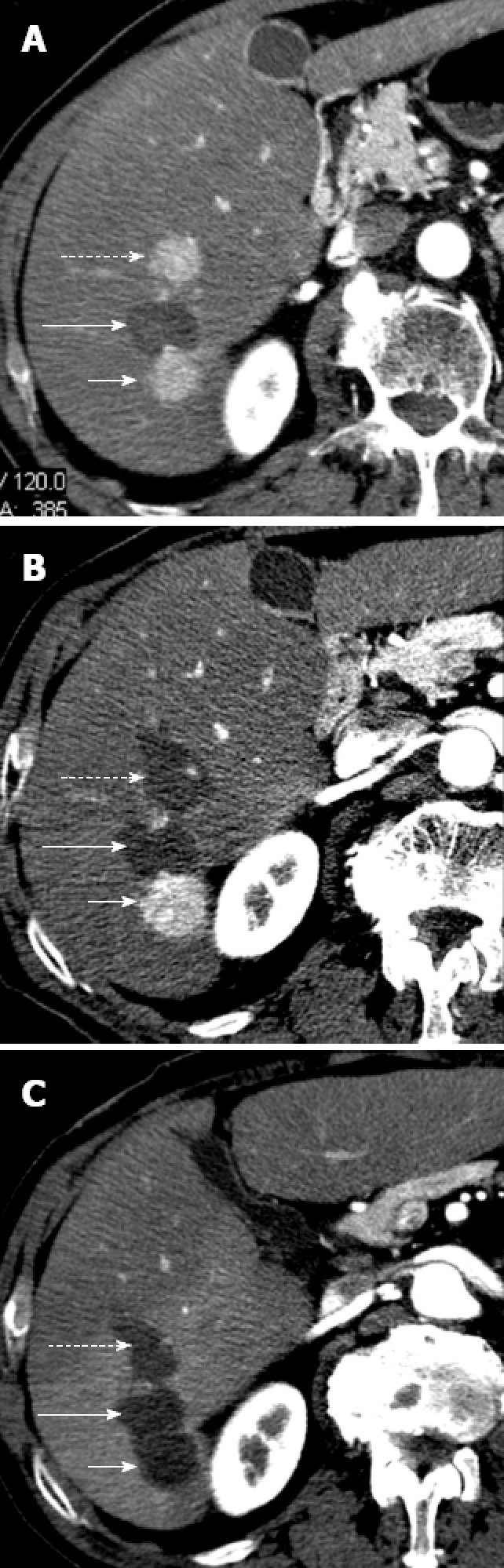
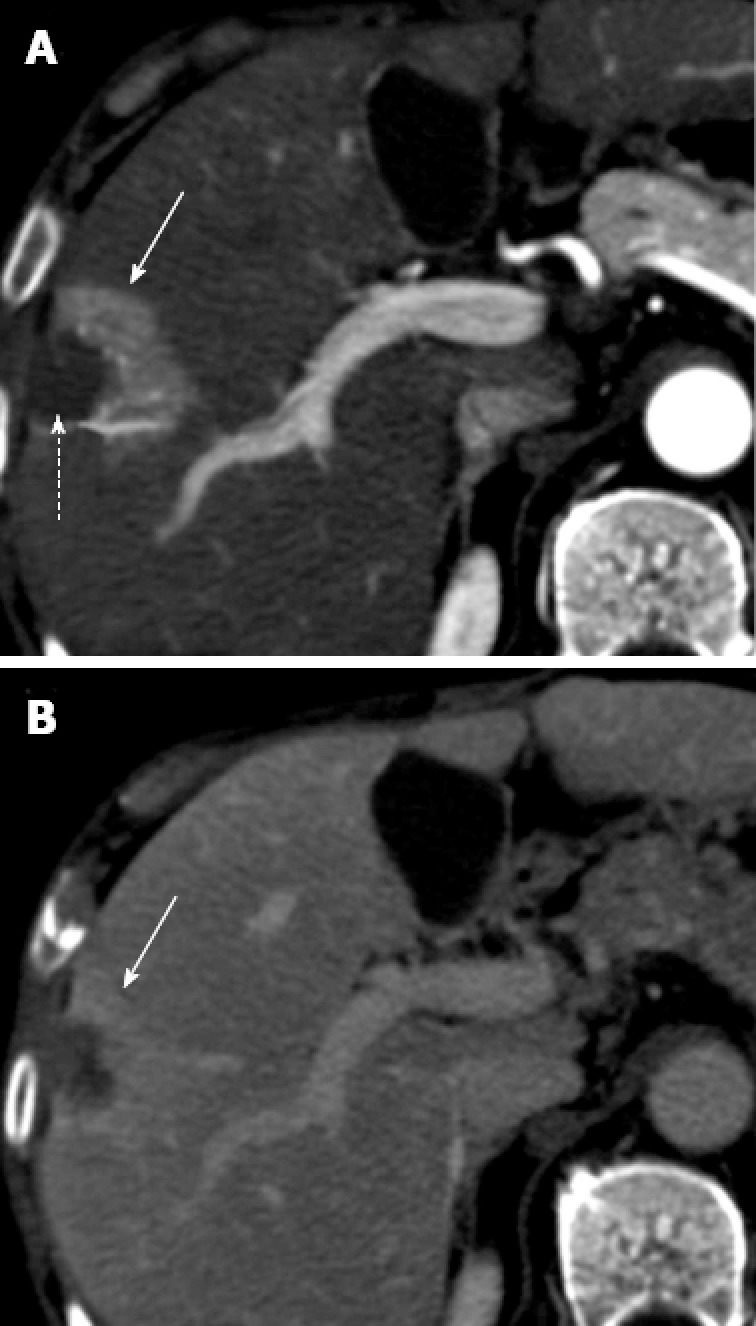
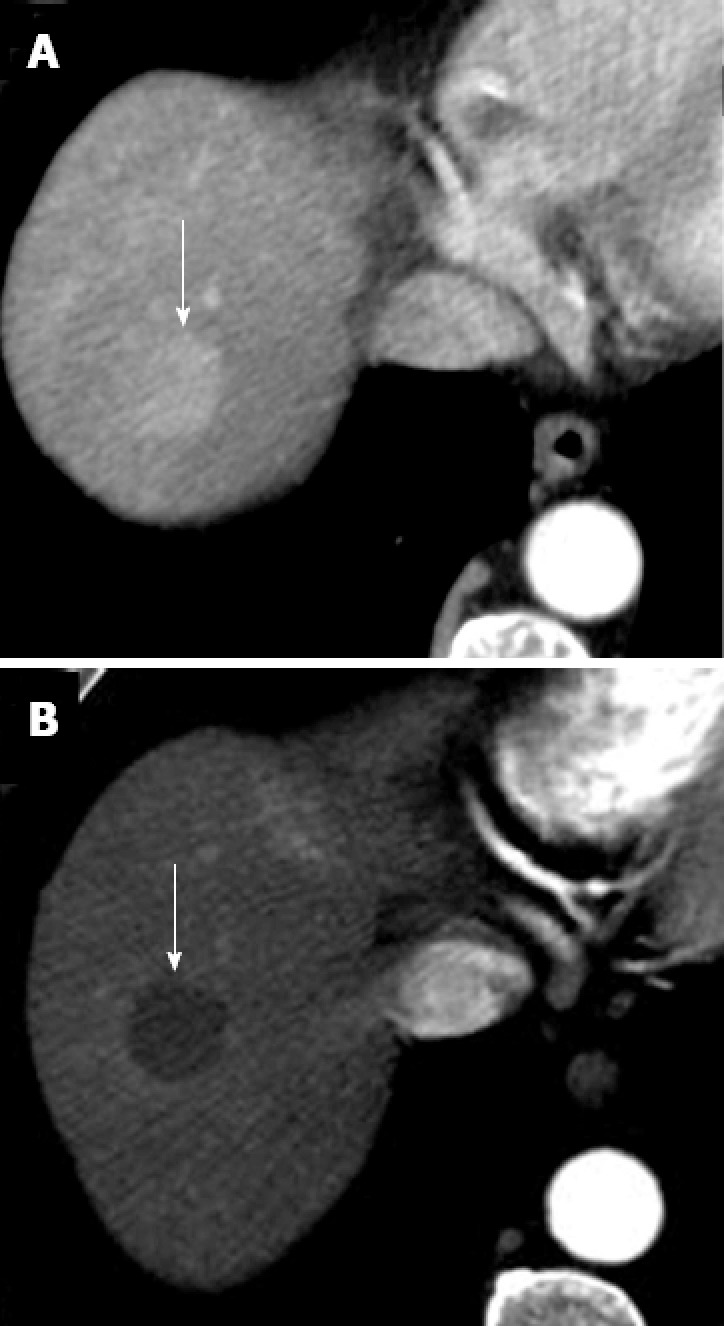
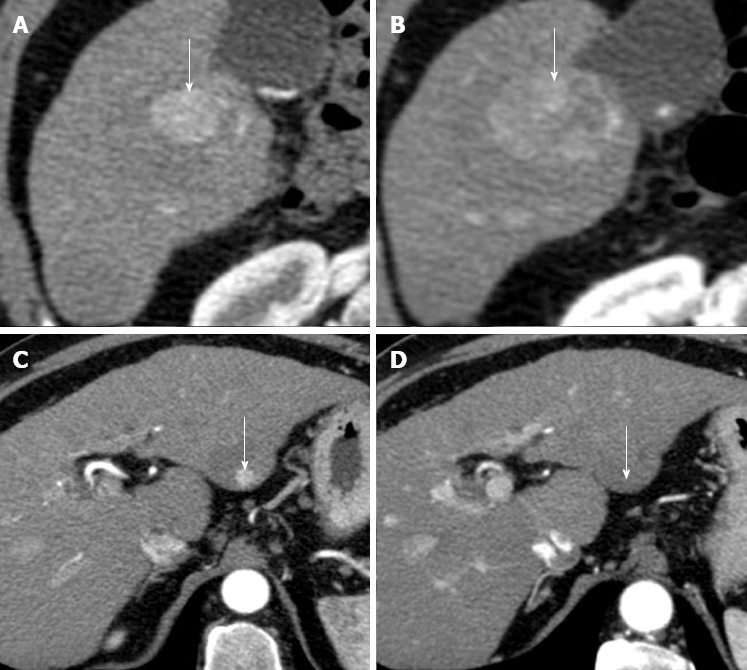
Surgical resection and imaging guided treatments play a crucial role in the management of hepatocellular carcinoma (HCC). Although the primary end point of treatment of HCC is survival, radiological response could be a surrogate end point of survival, and has a key role in HCC decision-making process. However, radiological assessment of HCC treatment efficacy is often controversial. There are few doubts on the evaluation of surgical resection; in fact, all known tumor sites should be removed. However, an unenhancing partial linear peripheral halo, in most cases, surrounding a fluid collection reducing in size during follow-up is demonstrated in successfully resected tumor with bipolar radiofrequency electrosurgical device. Efficacy assessment of locoregional therapies is more controversial and differs between percutaneous ablation (e.g., radiofrequency ablation and percutaneous ethanol injection) and transarterial treatments (e.g., conventional transarterial chemoembolization, transarterial chemoembolization with drug eluting beads and radioembolization). Finally, a different approach should be used for new systemic agent that, though not reducing tumor mass, could have a benefit on survival by delaying tumor progression and death. The purpose of this brief article is to review HCC imaging appearance after treatment.
Keywords: Hepatocellular carcinoma; Imaging; Treatment.
Figures

References
-
- Genco C, Cabibbo G, Maida M, Brancatelli G, Galia M, Alessi N, Butera G, Genova C, Romano P, Raineri M, et al. Treatment of hepatocellular carcinoma: present and future. Expert Rev Anticancer Ther. 2013;13:469–479. - PubMed
-
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378–390. - PubMed
-
- Iavarone M, Cabibbo G, Piscaglia F, Zavaglia C, Grieco A, Villa E, Cammà C, Colombo M. Field-practice study of sorafenib therapy for hepatocellular carcinoma: a prospective multicenter study in Italy. Hepatology. 2011;54:2055–2063. - PubMed
-
- Maida M, Cabibbo G, Brancatelli G, Genco C, Alessi N, Genova C, Romano P, Raineri M, Giarratano A, Midiri M, et al. Assessment of treatment response in hepatocellular carcinoma: a review of the literature. Future Oncol. 2013;9:845–854. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
