

Shared decision-making in antihypertensive therapy: a cluster randomised controlled trial
- PMID: 24024587
- PMCID: PMC3847233
- DOI: 10.1186/1471-2296-14-135
Shared decision-making in antihypertensive therapy: a cluster randomised controlled trial
Abstract
Background: Hypertension is one of the key factors causing cardiovascular diseases. A substantial proportion of treated hypertensive patients do not reach recommended target blood pressure values. Shared decision making (SDM) is to enhance the active role of patients. As until now there exists little information on the effects of SDM training in antihypertensive therapy, we tested the effect of an SDM training programme for general practitioners (GPs). Our hypotheses are that this SDM training (1) enhances the participation of patients and (2) leads to an enhanced decrease in blood pressure (BP) values, compared to patients receiving usual care without prior SDM training for GPs.
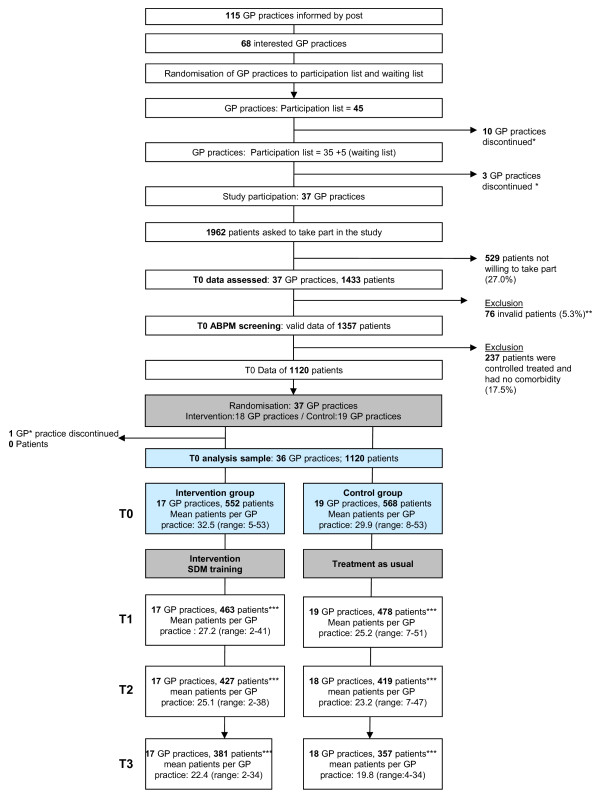
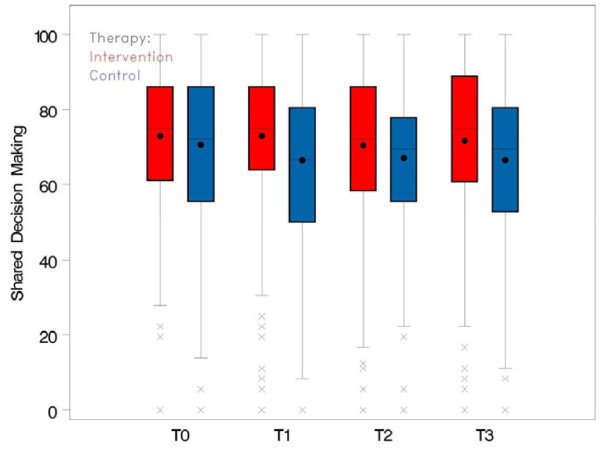
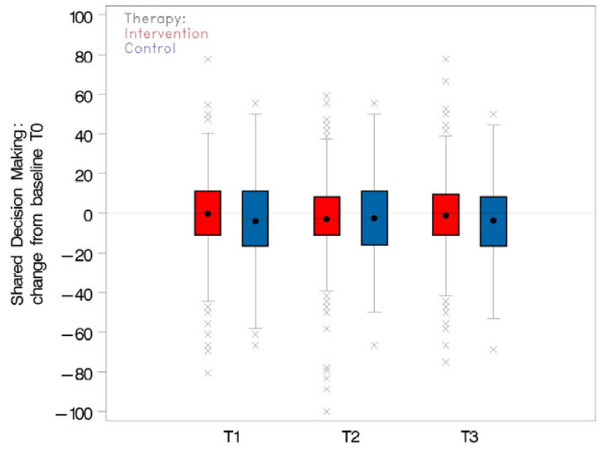
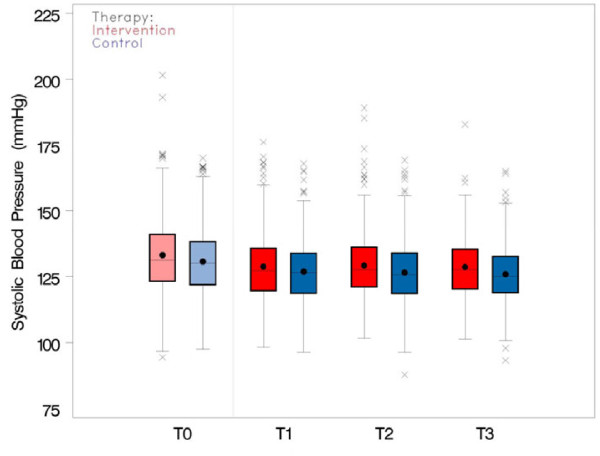
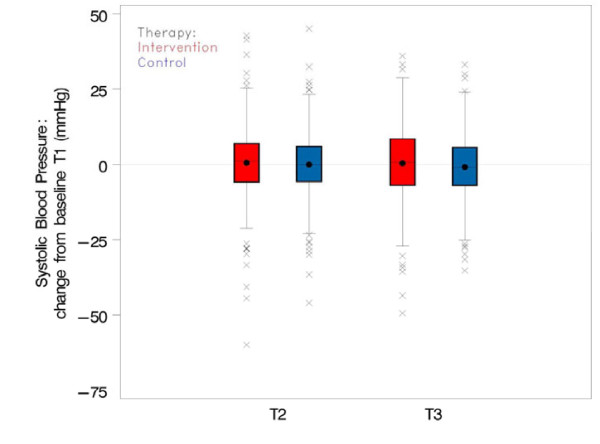
Methods: The study was conducted as a cluster randomised controlled trial (cRCT) with GP practices in Southwest Germany. Each GP practice included patients with treated but uncontrolled hypertension and/or with relevant comorbidity. After baseline assessment (T0) GP practices were randomly allocated into an intervention and a control arm. GPs of the intervention group took part in the SDM training. GPs of the control group treated their patients as usual. The intervention was blinded to the patients. Primary endpoints on patient level were (1) change of patients' perceived participation (SDM-Q-9) and (2) change of systolic BP (24h-mean). Secondary endpoints were changes of (1) diastolic BP (24h-mean), (2) patients' knowledge about hypertension, (3) adherence (MARS-D), and (4) cardiovascular risk score (CVR).
Results: In total 1357 patients from 36 general practices were screened for blood pressure control by ambulatory blood pressure monitoring (ABPM). Thereof 1120 patients remained in the study because of uncontrolled (but treated) hypertension and/or a relevant comorbidity. At T0 the intervention group involved 17 GP practices with 552 patients and the control group 19 GP practices with 568 patients. The effectiveness analysis could not demonstrate a significant or relevant effect of the SDM training on any of the endpoints.
Conclusion: The study hypothesis that the SDM training enhanced patients' perceived participation and lowered their BP could not be confirmed. Further research is needed to examine the impact of patient participation on the treatment of hypertension in primary care.
Trial registration: German Clinical Trials Register (DRKS): DRKS00000125.
Figures
References
-
- U.S. Department of Health and Human Services, National Institutes of Health, National Heart Lung and Blood Institute. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Full version. NIH Publication No 04–5230. 2004. pp. 1–88. [ http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf] (last accessed September 05, 2013) - PubMed
-
- Robert Koch Institute. Gesundheitsberichterstattung des Bundes [Federal Health Monitoring System] Berlin; 2009. Daten und Fakten: Ergebnisse der Studie “Gesundheit in Deutschland aktuell 2009” [Data and facts: Results of the study “Health in Germany 2009”] pp. 1–139. [in German, English abstract not available] http://www.gbe-bund.de/gbe10/owards.prc_show_pdf?p_id=13126&p_sprache=D (last accessed August 02, 2013)
-
- Ostchega Y, Dillon CF, Hughes JP, Carroll M, Yoon S. Trends in hypertension prevalence, awareness, treatment, and control in older U.S. adults: data from the National Health and Nutrition Examination Survey 1988 to 2004. J Am Geriatr Soc. 2007;55(7):1056–1065. doi: 10.1111/j.1532-5415.2007.01215.x. - DOI - PubMed
-
- Valderrama AL, Tong X, Ayala C, Keenan NL. Prevalence of self-reported hypertension, advice received from health care professionals, and actions taken to reduce blood pressure among US adults–HealthStyles, 2008. J Clin Hypertens. 2010;12(10):784–792. doi: 10.1111/j.1751-7176.2010.00323.x. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
