

Pregnancy characteristics and women's future cardiovascular health: an underused opportunity to improve women's health?
- PMID: 24025350
- PMCID: PMC3873841
- DOI: 10.1093/epirev/mxt006
Pregnancy characteristics and women's future cardiovascular health: an underused opportunity to improve women's health?
Abstract
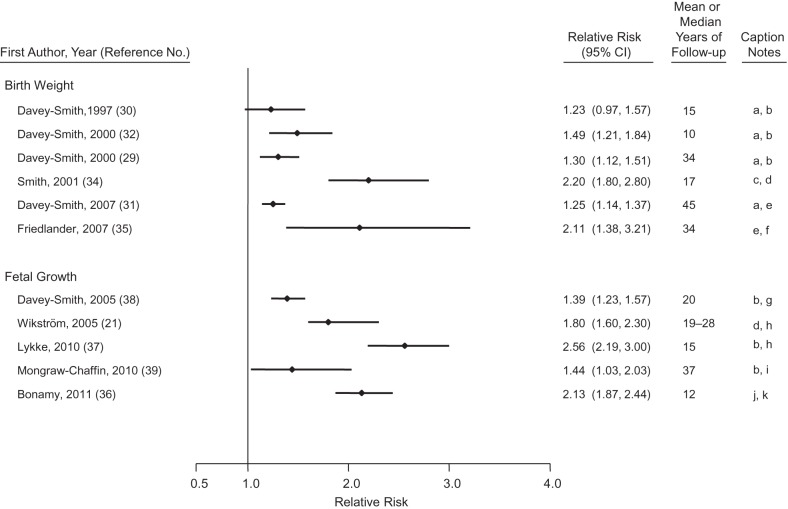
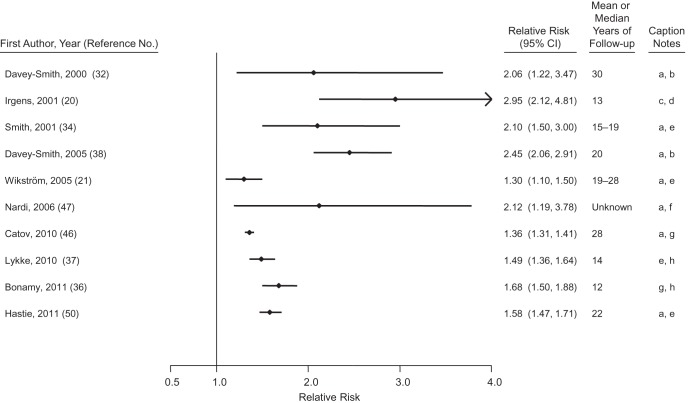
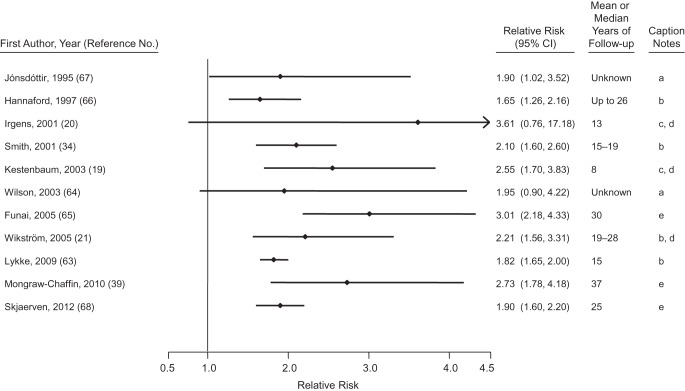
Growing evidence indicates that women with a history of common pregnancy complications, including fetal growth restriction and preterm delivery (often combined as low birth weight), hypertensive disorders of pregnancy, and gestational diabetes, are at increased risk for cardiovascular disease later in life. The purpose of this paper was to review the associations of parity and these 4 pregnancy complications with cardiovascular morbidity and mortality; to review the role of cardiovascular risk factors before, during, and after pregnancy complications in explaining these associations; and to explore the implications of this emerging science for new research and policy. We systematically searched for relevant cohort and case-control studies in Medline through December 2012 and used citation searches for already published reviews to identify new studies. The findings of this review suggest consistent and often strong associations of pregnancy complications with latent and future cardiovascular disease. Many pregnancy complications appear to be preceded by subclinical vascular and metabolic dysfunction, suggesting that the complications may be useful markers of latent high-risk cardiovascular trajectories. With further replication research, these findings would support the utility of these prevalent pregnancy complications in identifying high-risk women for screening, prevention, and treatment of cardiovascular disease, the leading cause of morbidity and mortality among women.
Keywords: birth weight; cardiovascular disease; diabetes, gestational; preeclampsia; pregnancy; premature birth; women's health.
Figures

References
-
- Rich-Edwards JW. Reproductive health as a sentinel of chronic disease in women. Womens Health (Lond Engl) 2009;5(2):101–105. - PubMed
-
- Decline in deaths from heart disease and stroke—United States, 1900–1999. MMWR Morb Mortal Wkly Rep. 1999;48(30):649–656. - PubMed
-
- Yusuf S, Reddy S, Ôunpuu S, et al. Global burden of cardiovascular diseases. Circulation. 2001;104(22):2746–2753. - PubMed
-
- Shah RU, Klein L, Lloyd-Jones DM. Heart failure in women: epidemiology, biology and treatment. Womens Health (Lond Engl) 2009;5(5):517–527. - PubMed
-
- Mathers C, Boerma JT, Fat DM, et al. The Global Burden of Disease: 2004 Update. Geneva, Switzerland: World Health Organization; 2008.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
