

Standardization of T1 measurements with MOLLI in differentiation between health and disease--the ConSept study
- PMID: 24025486
- PMCID: PMC3847466
- DOI: 10.1186/1532-429X-15-78
Standardization of T1 measurements with MOLLI in differentiation between health and disease--the ConSept study
Abstract
Background: T1 imaging based on pixel-wise quantification of longitudinal relaxation has the potential to differentiate between normal and abnormal myocardium. The accuracy of T1 measurement has not been established nor systematically tested in the presence of health and disease.
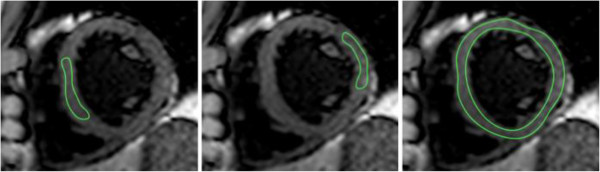
Methods: Intra-observer, inter-observer and inter-study reproducibility of T1 imaging was assessed in subjects with left ventricular hypertrophy (LVH, n = 25) or dilated cardiomyopathy (DCM, n = 43). Thirty-eight subjects with low-pretest likelihood of cardiomyopathy served as a control group. T1 values were acquired in a single mid-ventricular short axis slice using modified Look-Locker imaging prior and after the application of gadolinium contrast at 1.5 and 3 T. Analysis was performed with regions of interest (ROI) placed conservatively within the septum or to include the whole short axis (SAX) myocardium.
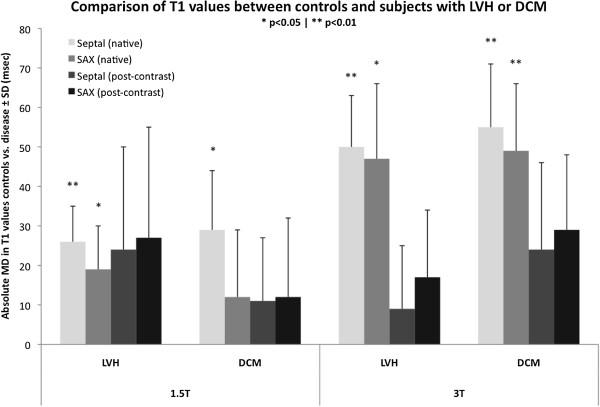
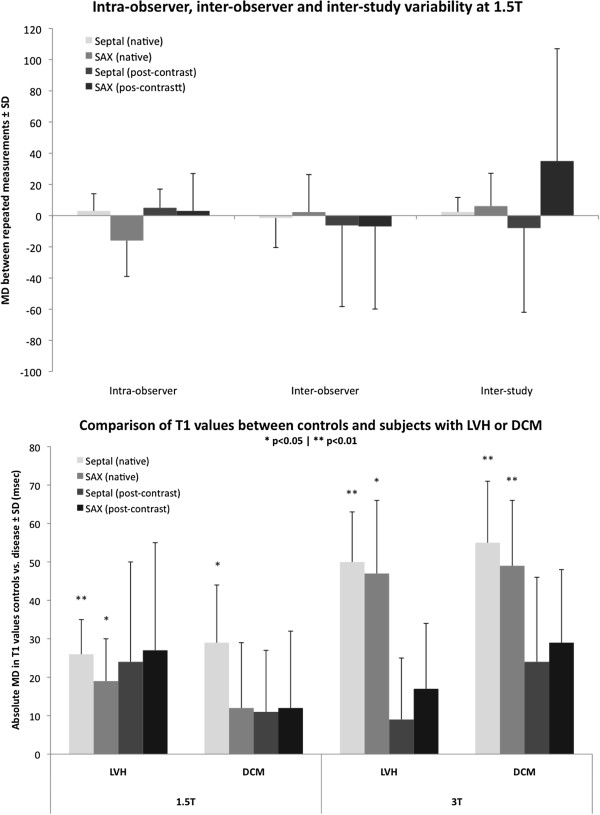
Results: Intra-observer, inter-observer and inter-study repeated measurements within the septum showed smaller mean differences and narrower 95% confidence intervals than repeated short axis ROI measurements. Native T1 values were higher in septal ROIs compared with SAX values at both field strengths (1.5 T: 976 ± 37 vs. 952 ± 41, p < 0.01; 3 T: 1108 ± 67 vs. 1087 ± 60, p < 0.01). Native T1 values revealed significant mean differences between controls and patients with LVH for both septal (1.5 T: 26 ± 9, p < 0.01; 3 T: 50 ± 13, p < 0.01) and SAX ROIs (1.5 T: 19 ± 11, p < 0.05; 3 T: 47 ± 19, p < 0.05) with greater differences observed at 3 T versus 1.5 T field strength. Native T1 values revealed significant mean differences between controls and patients with DCM for septal ROI (1.5 T: 29 ± 15, p < 0.05; 3 T: 55 ± 16, p < 0.01) at both 1.5 T and 3 T, but only for SAX ROIs at 3 T (49 ± 17, p < 0.01). There were no significant differences in post-contrast T1 values or partition coefficient (λ) between controls and patients.
Conclusion: Conservative septal ROI T1 measurement is a robust technique with excellent intra-observer, inter-observer and inter-study reproducibility for native and post-contrast T1 value and partition coefficient measurements. Moreover, native septal T1 values reveal the greatest difference between normal and abnormal myocardium, which is independent of geometrical alterations of cardiac chamber and wall thickness. We propose the use of native T1 measurements using conservative septal technique as the standardized approach to distinguish health from disease assuming diffuse myocardial involvement.
Figures
References
-
- Pastor A, Voigt T, Schaffter T, Nagel E, Puntmann VO. Usefulness of cardiac magnetic resonance in early assessment of cardiomyopathies: myocardial fibrosis is a common denominator. Curr Cardiovasc Imag Rep. 2012;2:77–82.
-
- Puntmann VO, Voigt T, Chen Z, Mayr M, Karim R, Rhode K, Pastor A, Carr-White G, Razavi R, Schaeffter T, Nagel E. T1 mapping in differentiation of normal myocardium from diffuse disease in hypertrophic and dilated cardiomyopathy. JACC Cardiovasc Imag. 2013;6:475–84. doi: 10.1016/j.jcmg.2012.08.019. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
