

Renal tumors: diagnostic and prognostic biomarkers
- PMID: 24025522
- PMCID: PMC4714713
- DOI: 10.1097/PAS.0b013e318299f12e
Renal tumors: diagnostic and prognostic biomarkers
Abstract
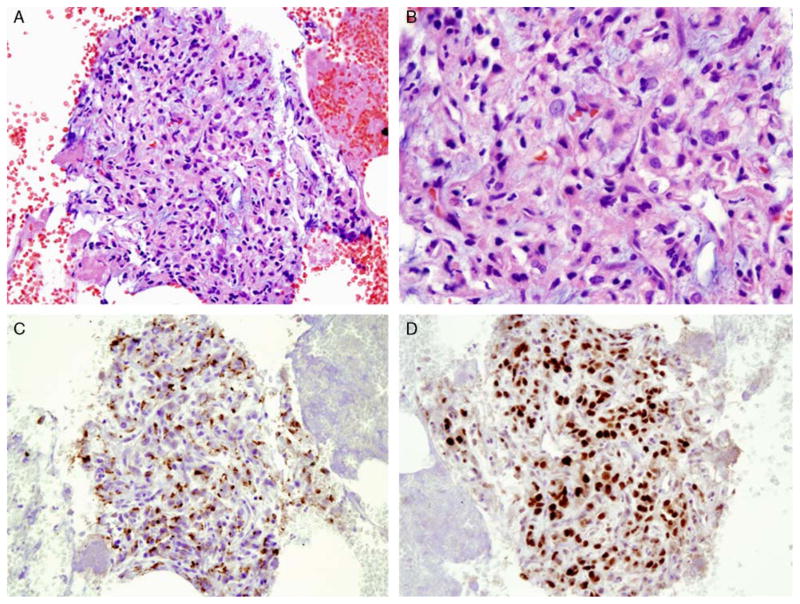
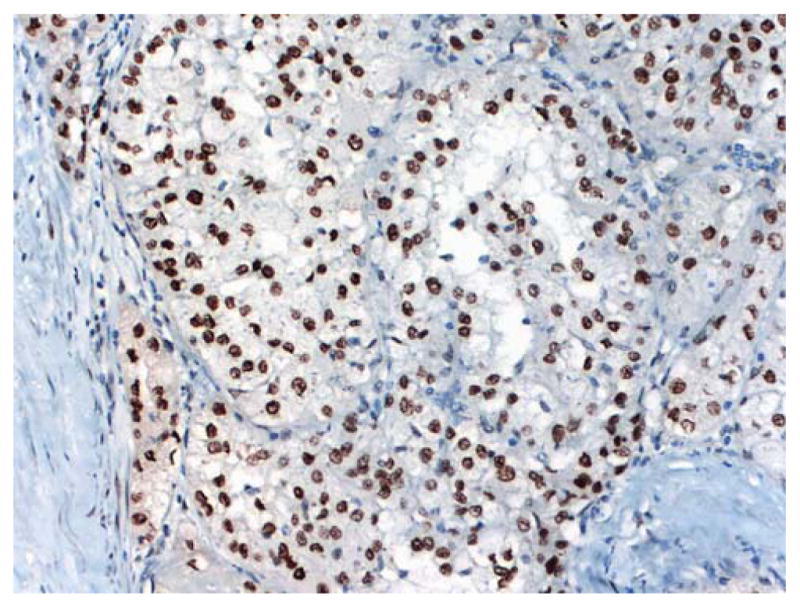
The International Society of Urological Pathology convened a consensus conference on renal cancer, preceded by an online survey, to address issues relating to the diagnosis and reporting of renal neoplasia. In this report, the role of biomarkers in the diagnosis and assessment of prognosis of renal tumors is addressed. In particular we focused upon the use of immunohistochemical markers and the approach to specific differential diagnostic scenarios. We enquired whether cytogenetic and molecular tools were applied in practice and asked for views on the perceived prognostic role of biomarkers. Both the survey and conference voting results demonstrated a high degree of consensus in participants' responses regarding prognostic/predictive markers and molecular techniques, whereas it was apparent that biomarkers for these purposes remained outside the diagnostic realm pending clinical validation. Although no individual antibody or panel of antibodies reached consensus for classifying renal tumors, or for confirming renal metastatic disease, it was noted from the online survey that 87% of respondents used immunohistochemistry to subtype renal tumors sometimes or occasionally, and a majority (87%) used immunohistochemical markers (Pax 2 or Pax 8, renal cell carcinoma [RCC] marker, panel of pan-CK, CK7, vimentin, and CD10) in confirming the diagnosis of metastatic RCC. There was consensus that immunohistochemistry should be used for histologic subtyping and applied before reaching a diagnosis of unclassified RCC. At the conference, there was consensus that TFE3 and TFEB analysis ought to be requested when RCC was diagnosed in a young patient or when histologic appearances were suggestive of the translocation subtype; whereas Pax 2 and/or Pax 8 were considered to be the most useful markers in the diagnosis of a renal primary.
Figures





References
-
- Delahunt B, Egevad L, Montironi R, et al. International Society of Urological Pathology (ISUP) consensus conference on renal neoplasia: rationale and organization. Am J Surg Pathol. 2013 - PubMed
-
- Truong LD, Shen SS. Immunohistochemical diagnosis of renal neoplasms. Arch Pathol Lab Med. 2011;135:92–109. - PubMed
-
- Skinnider BF, Amin MB. An immunohistochemical approach to the differential diagnosis of renal tumors. Semin Diagn Pathol. 2005;22:51–68. - PubMed
-
- Eble JN, Sauter G, Epstein JI, et al. Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs. WHO Classification of Tumours. Lyon: IARC Press; 2004. pp. 10–43.
-
- Tickoo SK, Reuter VE. Differential diagnosis of renal tumors with papillary architecture. Adv Anat Pathol. 2011;18:120–132. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
