

Paratesticular fibrous pseudotumor in young males presenting with histological features of IgG4-related disease: two case reports
- PMID: 24025610
- PMCID: PMC3848042
- DOI: 10.1186/1752-1947-7-225
Paratesticular fibrous pseudotumor in young males presenting with histological features of IgG4-related disease: two case reports
Abstract
Introduction: Paratesticular fibrous pseudotumors represent benign new growths confined to intrascrotal structures. Both pathogenesis and clinical management are little understood due to the rarity of the lesion, with less than 200 cases reported to date. Recently, paratesticular fibrous pseudotumors have been postulated to be immunoglobulin G4-related, pathogenetically. Here we report two cases of patients with paratesticular fibrous pseudotumor to highlight the clinical features of this rare disease and we report the immunohistochemical examinations to support the theory of paratesticular fibrous pseudotumor being an immunoglobulin G4-related disease.
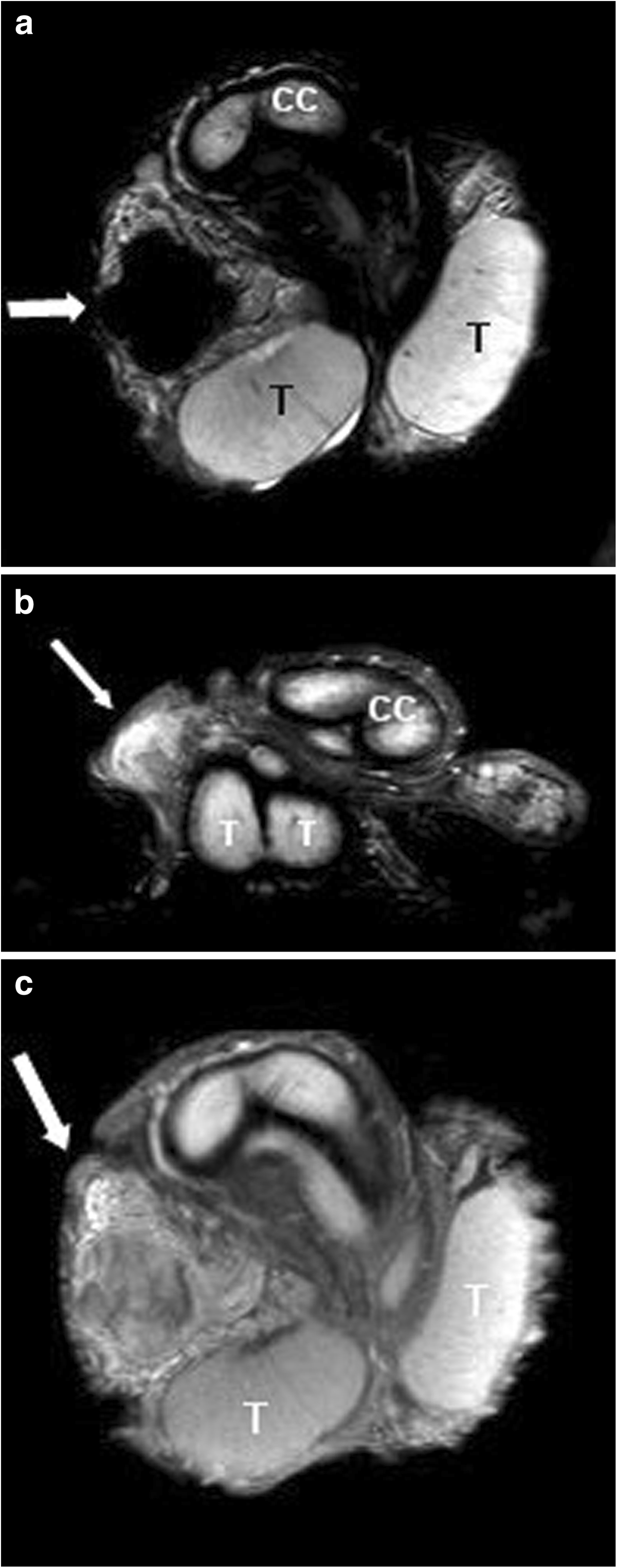
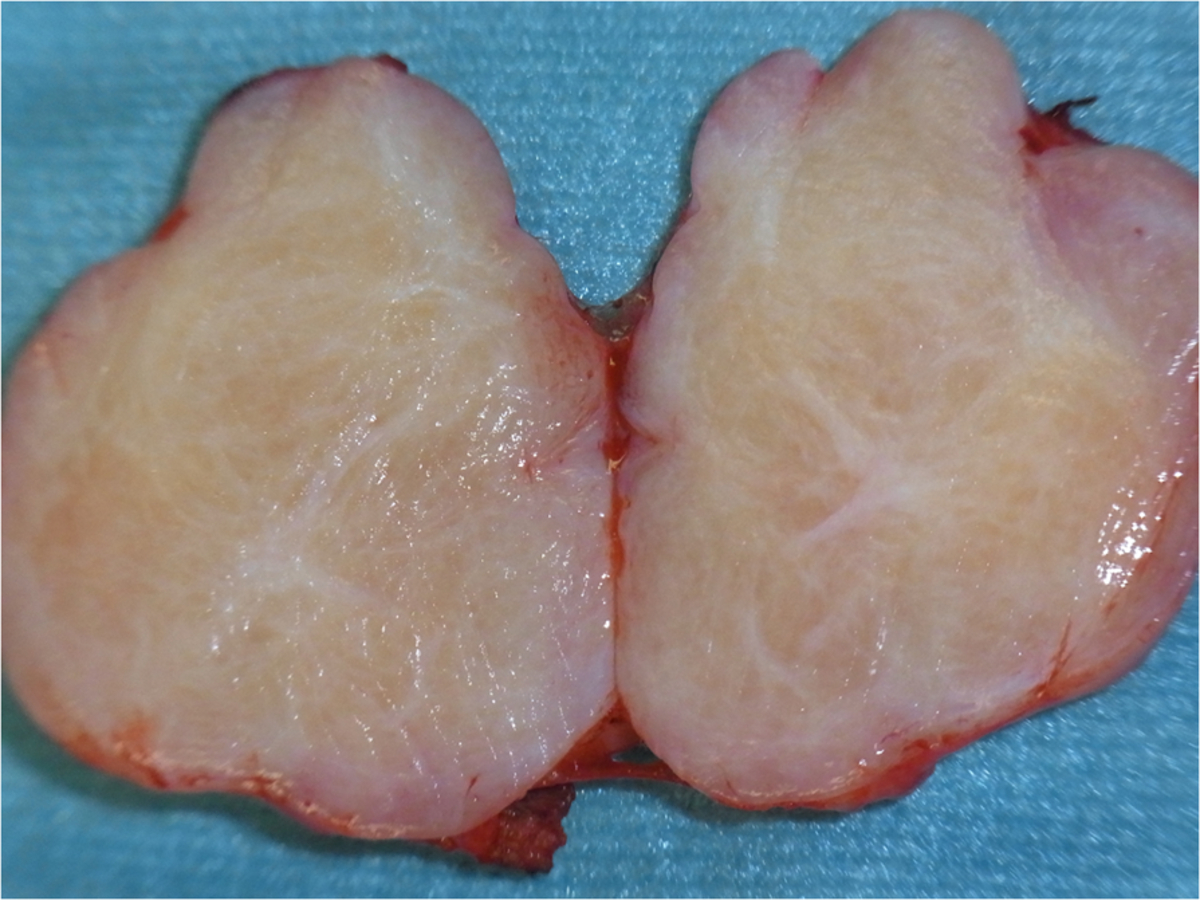
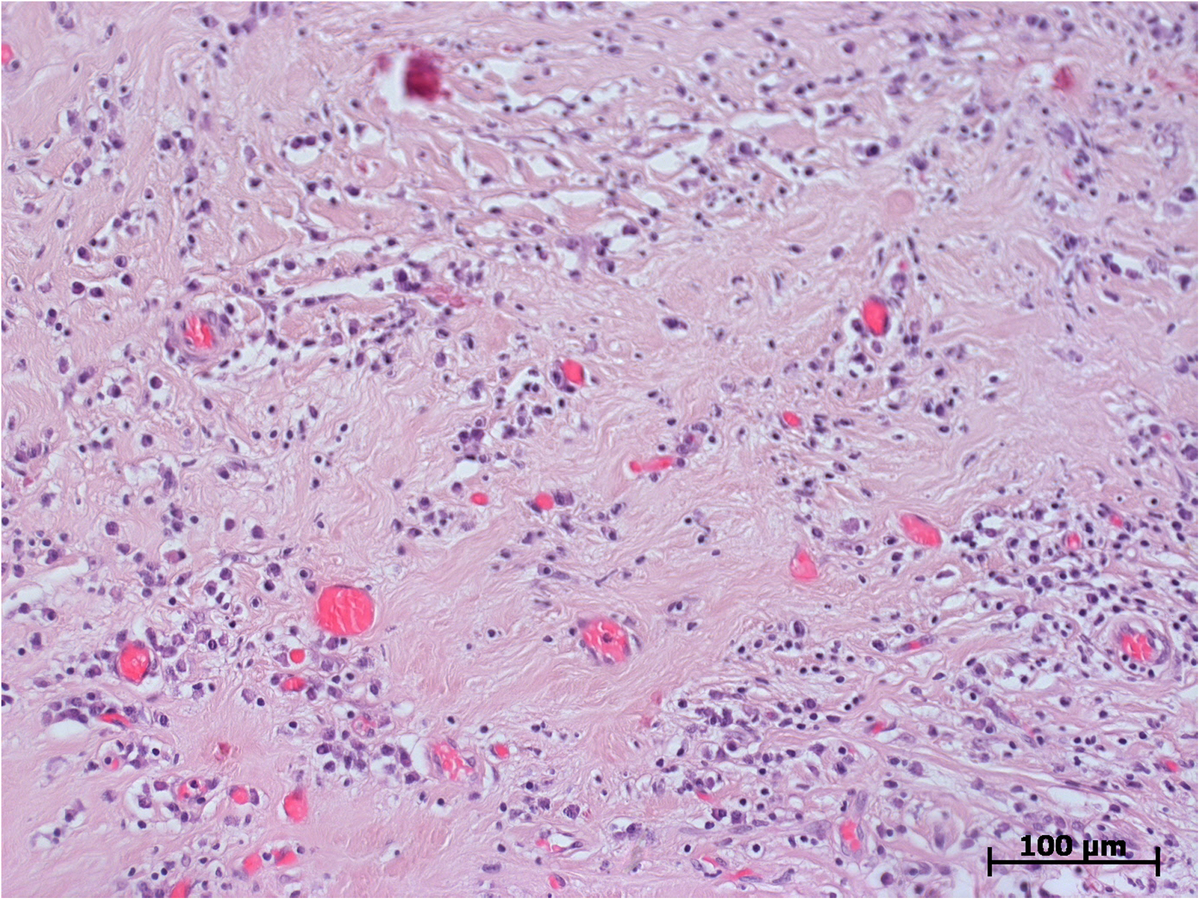
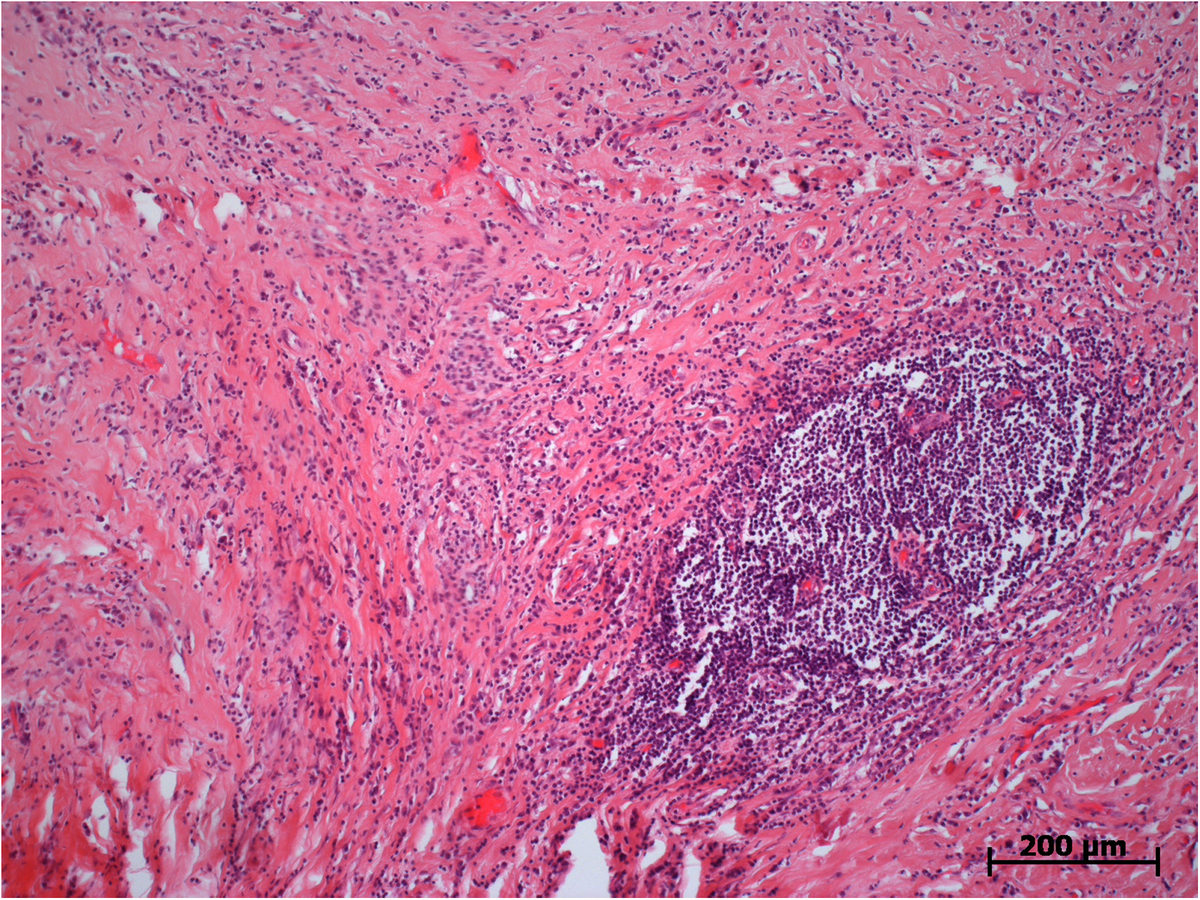
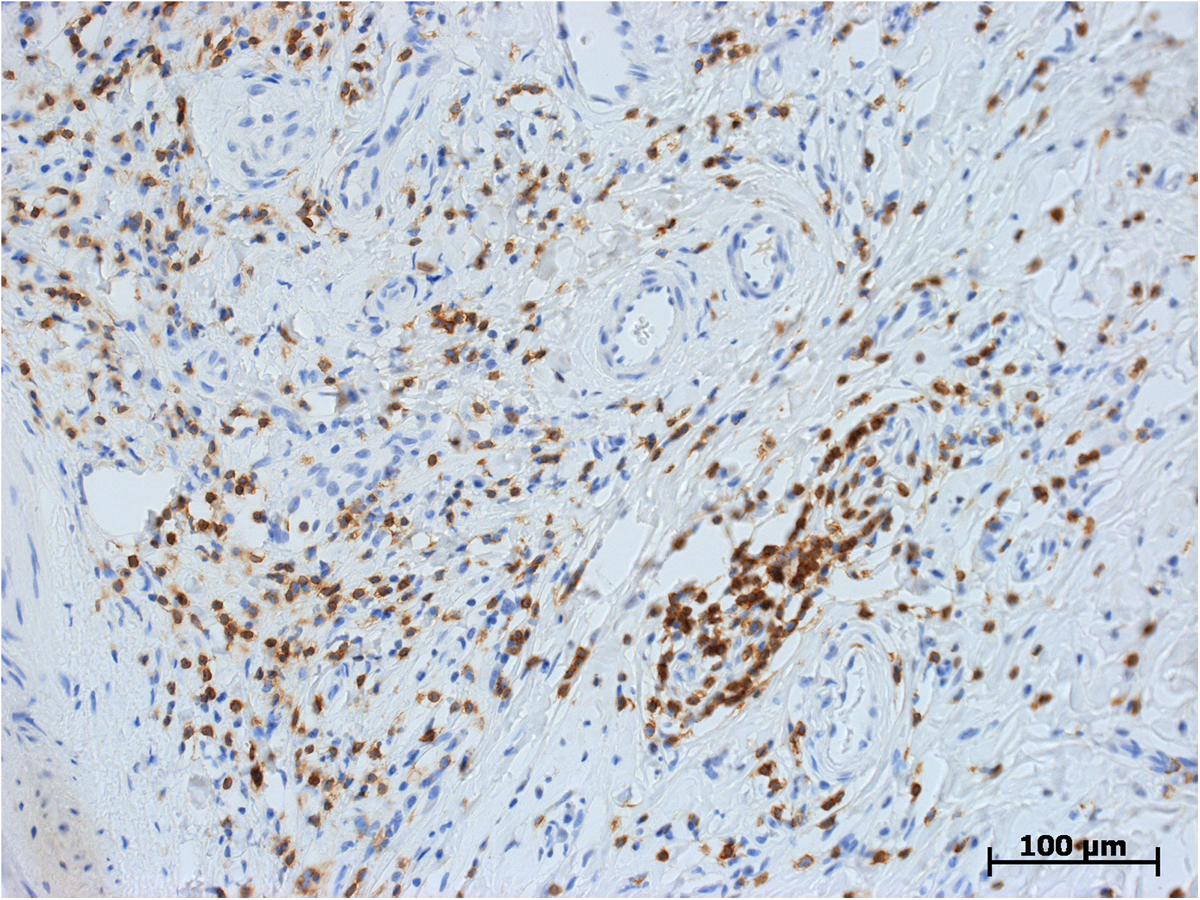
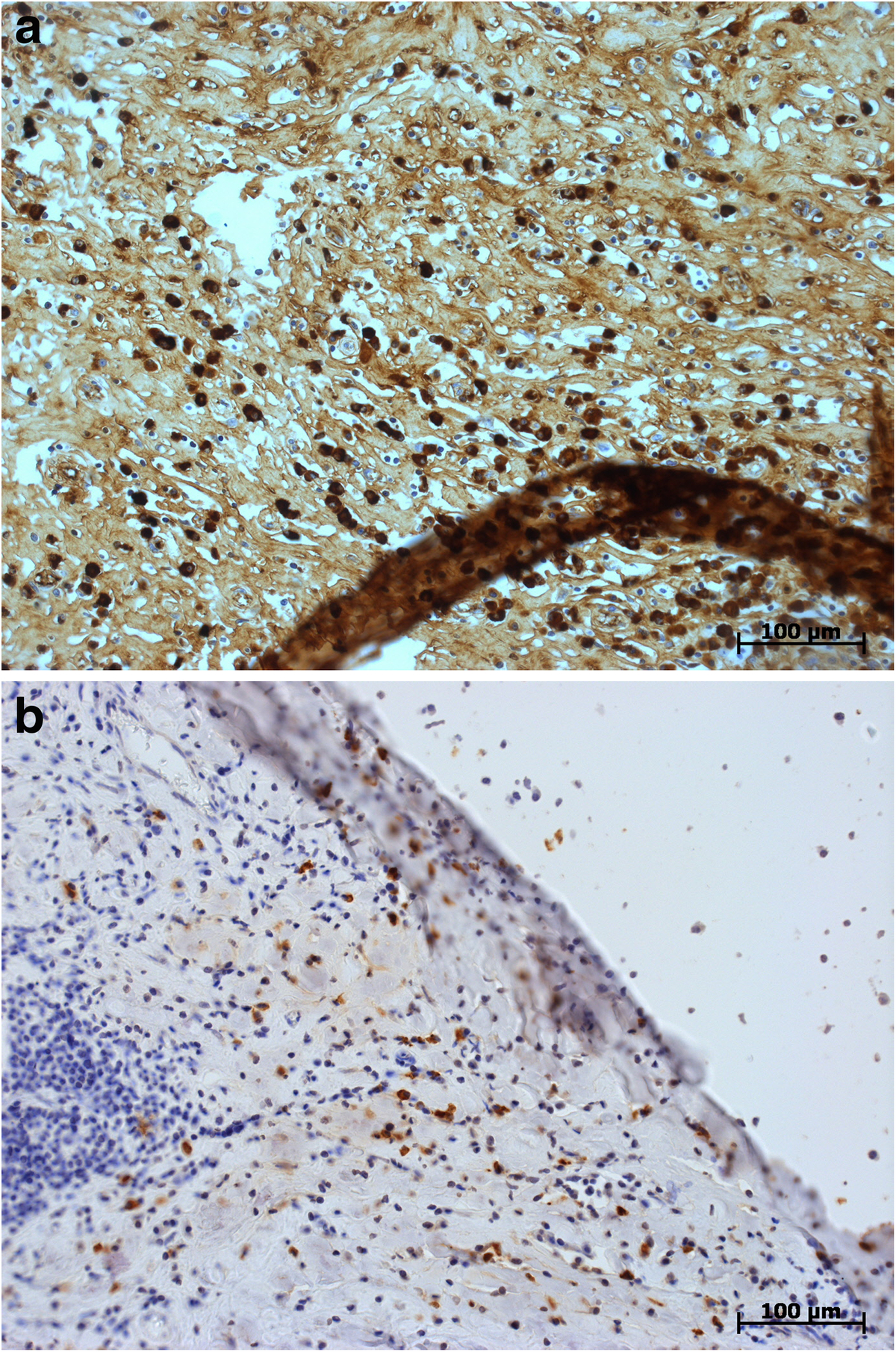
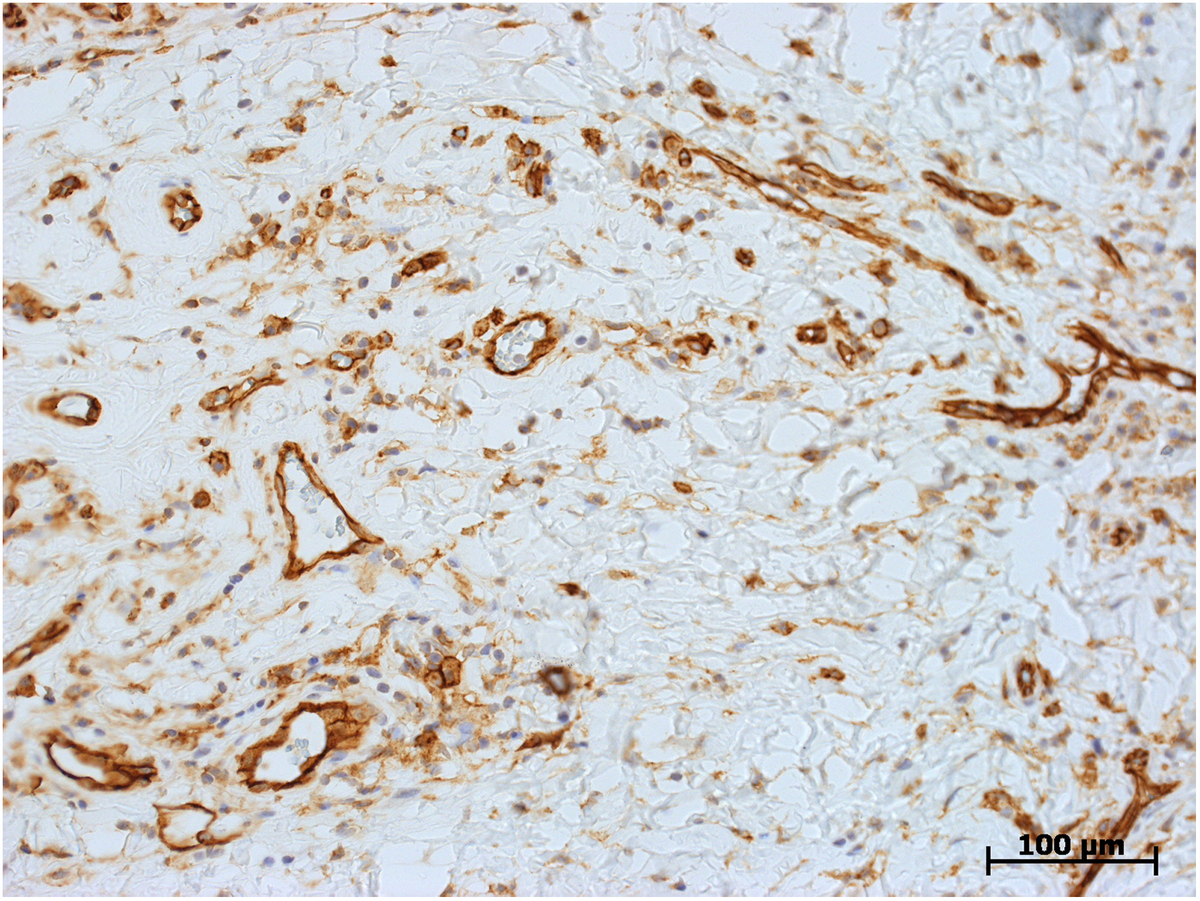
Case presentations: A 28-year-old white man presented with a painless intrascrotal mass. After a clinical examination, a malignant growth was suspected. His ultrasound results revealed a well-demarcated hypoechoic lesion of 1.5cm in diameter at the spermatic cord. Our patient underwent local excision. His follow-up has been uneventful for 12 years. The second case was an 18-year-old white man who presented with a painless scrotal mass suspicious of testicular tumor. A magnetic resonance imaging scan revealed a 3cm mass at the spermatic cord with very low signal density on T2-weighted imaging and a low and inhomogeneous uptake of gadolinium contrast agent on T1-weighted, fat-suppressed imaging. Following local excision, our patient has been well for 18 months.On histological examination, both of the lesions consisted of collagen-rich hyalinized fibrotic tissue with storiform features. There were lymphofollicular infiltrates and, sporadically, also venulitis. The immunoglobulin G4 staining (in case 2) showed an infiltrate of 10 to 15 positive cells per high-power field on average, corresponding to a proportion of 40% in evaluable hot spots. The two patients with paratesticular fibrous pseudotumor presented within a time span of 15 years. During that time, 400 patients with testicular germ cell tumors had been treated in our institution.
Conclusions: The specific histological features documented in our case lend support to the theory of paratesticular fibrous pseudotumor being an immunoglobulin G4-related sclerosing disorder. Paratesticular fibrous pseudotumors usually occur in young adulthood. Clinically, paratesticular fibrous pseudotumor can mimic testicular malignancy. Ultrasonographic findings are largely unspecific, however, scrotal magnetic resonance imaging may aid in discriminating the lesion from malignant tumors. Local excision, whenever technically feasible, is the preferred treatment of paratesticular fibrous pseudotumor.
Figures


Similar articles
-
Paratesticular Fibrous Pseudotumor: A New Entity of IgG4-Related Disease?Ann Clin Lab Sci. 2018 May;48(3):381-385. Ann Clin Lab Sci. 2018. PMID: 29970445
-
Left paratesticular fibrous pseudotumor on the single testis and contribution of imaging in therapeutic management, a case report.Int J Surg Case Rep. 2023 Apr;105:108077. doi: 10.1016/j.ijscr.2023.108077. Epub 2023 Mar 28. Int J Surg Case Rep. 2023. PMID: 36996707 Free PMC article.
-
Paratesticular Fibrous Pseudotumor in a Pediatric Patient: A Case Report.Cureus. 2024 Oct 14;16(10):e71453. doi: 10.7759/cureus.71453. eCollection 2024 Oct. Cureus. 2024. PMID: 39539915 Free PMC article.
-
Paratesticular fibrous pseudotumor: a report of five cases and literature review.Front Med. 2014 Dec;8(4):484-8. doi: 10.1007/s11684-014-0325-3. Epub 2014 Mar 14. Front Med. 2014. PMID: 24627288 Review.
-
A case of fibrous pseudotumor originating from tunica vaginalis testis.Hinyokika Kiyo. 2005 Jul;51(7):483-6. Hinyokika Kiyo. 2005. PMID: 16119816 Review.
Cited by
-
Retroperitoneal disorders associated with IgG4-related autoimmune pancreatitis.World J Gastroenterol. 2014 Nov 28;20(44):16550-8. doi: 10.3748/wjg.v20.i44.16550. World J Gastroenterol. 2014. PMID: 25469023 Free PMC article. Review.
-
IgG4-Related Disease with Selective Testicular Involvement- A Rare Entity: Case Report with Review of Literature.Turk Patoloji Derg. 2021;37(1):78-83. doi: 10.5146/tjpath.2020.01493. Turk Patoloji Derg. 2021. PMID: 32525212 Free PMC article. Review.
-
Neoplastic diseases of the spermatic cord: an overview of pathological features, evaluation, and management.Transl Androl Urol. 2017 Feb;6(1):101-110. doi: 10.21037/tau.2017.01.04. Transl Androl Urol. 2017. PMID: 28217455 Free PMC article. Review.
-
Paratesticular fibrous pseudotumor with histological features of IgG4-related disease: two case reports and review of the literature.Gland Surg. 2023 Mar 31;12(3):426-431. doi: 10.21037/gs-22-290. Epub 2023 Mar 3. Gland Surg. 2023. PMID: 37057041 Free PMC article.
-
Paratesticular fibrous pseudotumour: Intraoperative frozen section analysis can help prevent unnecessary orchiectomy.Can Urol Assoc J. 2015 Sep-Oct;9(9-10):E731-3. doi: 10.5489/cuaj.3110. Epub 2015 Oct 13. Can Urol Assoc J. 2015. PMID: 26664509 Free PMC article.
References
-
- Mostofi FK, Price EB. In: Atlas of tumor pathology. 2nd series, fascicle 8. Firminger HI, editor. Washington DC: Armed Forces Institute of Pathology; 1973. Tumors of the male genital system; pp. 151–154.
LinkOut - more resources
Full Text Sources
Other Literature Sources
