

Effects of dual blockade of the renin-angiotensin system on renal and cardiovascular outcomes in type 2 diabetes with overt nephropathy and hypertension in the ORIENT: a post-hoc analysis (ORIENT-Hypertension)
- PMID: 24026038
- PMCID: PMC3853587
- DOI: 10.1038/hr.2013.86
Effects of dual blockade of the renin-angiotensin system on renal and cardiovascular outcomes in type 2 diabetes with overt nephropathy and hypertension in the ORIENT: a post-hoc analysis (ORIENT-Hypertension)
Abstract
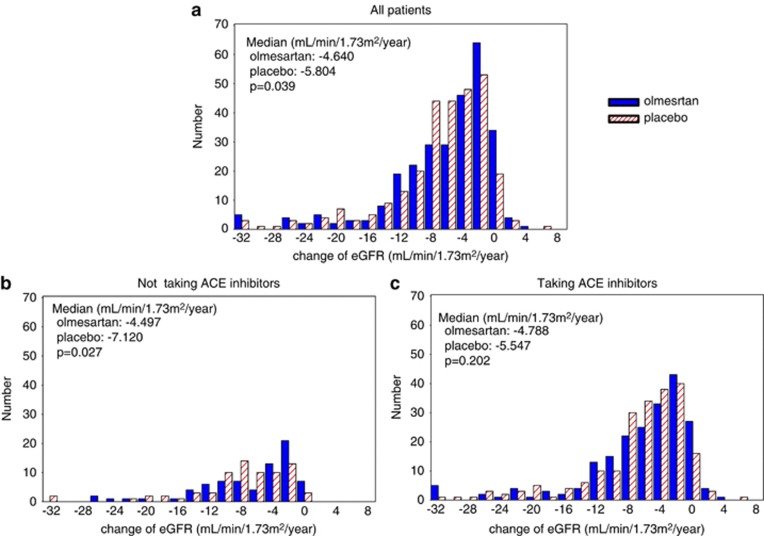
Combination therapy with angiotensin II receptor blockers and angiotensin-converting enzyme inhibitors (ACEIs) requires further evaluation in patients with diabetic nephropathy and hypertension. In a post hoc analysis of the Olmesartan Reducing Incidence of Endstage renal disease in diabetic Nephropathy Trial with hypertension, we examined the effects of olmesartan on renal and cardiovascular outcomes in the presence or absence of an ACEI. Among 563 patients randomized to receive either olmesartan (n = 280) or placebo (n = 283), 73.5% (n = 414) received a concomitant ACEI. Compared with placebo, olmesartan significantly reduced proteinuria in both the ACEI-treated and non-ACEI-treated groups. The respective changes in the urinary protein creatinine ratio in the olmesartan-treated and placebo-treated groups were -32.6% and +21.1% without an ACEI (P = 0.001) and -17.0% and +2.2% with an ACEI (P = 0.028). In the olmesartan group, 115 patients developed primary renal outcomes (41.1%) compared with 129 (45.6%) in the placebo group (hazard ratio (HR): 0.97, P = 0.787). The respective HRs in the ACEI-treated and non-ACEI-treated groups were 1.02 (P = 0.891) and 0.84 (P = 0.450). 40 olmesartan-treated patients (14.3%) and 53 placebo-treated patients (18.7%) developed secondary cardiovascular outcomes (HR: 0.65, P = 0.042). The respective HRs in the ACEI-treated and non-ACEI-treated groups were 0.69 (P = 0.129) and 0.51 (P = 0.129). Olmesartan was well tolerated. Dual blockade treatment caused more hyperkalemia than monotherapy. In patients with diabetic nephropathy and hypertension, olmesartan significantly reduced proteinuria, independent of ACEI treatment and cardiovascular outcome but failed to show additional renal benefit compared with ACEI treatment alone. The cardiovascular benefit of dual treatment requires further evaluation.
Figures




Comment in
-
Can two be better than one? Dual RAS blockade in patients with type 2 diabetes and overt nephropathy in the age of ONTARGET and ALTITUDE.Hypertens Res. 2014 Jan;37(1):4-6. doi: 10.1038/hr.2013.91. Epub 2013 Sep 12. Hypertens Res. 2014. PMID: 24026039 No abstract available.
References
-
- Excerpts From the United States Renal Data System 2008 Annual Data Report: international comparison. Am J Kidney Dis. 2009;53 (Suppl 1:S297–S308. - PubMed
-
- Bilous R. Microvascular disease: what does the UKPDS tell us about diabetic nephropathy. Diabet Med. 2008;25 (Suppl 2:25–29. - PubMed
-
- Bakris GL, Williams M, Dworkin L, Elliott WJ, Epstein M, Toto R, Tuttle K, Douglas J, Hsueh W, Sowers J. Preserving renal function in adults with hypertension and diabetes: a consensus approach. National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Am J Kidney Dis. 2000;36:646–661. - PubMed
-
- Ruggenenti P, Fassi A, Ilieva AP, Bruno S, Iliev IP, Brusegan V, Rubis N, Gherardi G, Arnoldi F, Ganeva M, Ene-Iordache B, Gaspari F, Perna A, Bossi A, Trevisan R, Dodesini AR, Remuzzi G. Preventing microalbuminuria in type 2 diabetes. N Engl J Med. 2004;351:1941–1951. - PubMed
-
- Haller H, Ito S, Izzo JL, Jr, Januszewicz A, Katayama S, Menne J, Mimran A, Rabelink TJ, Ritz E, Ruilope LM, Rump LC, Viberti G, ROADMAP Trial Investigators Olmesartan for the delay or prevention of microalbuminuria in type 2 diabetes. N Engl J Med. 2011;364:907–917. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical