

Design of the Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST)
- PMID: 24026162
- PMCID: PMC4536980
- DOI: 10.1097/01.brs.0000435048.23726.3e
Design of the Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST)
Abstract
Study design: Descriptive.
Objective: To describe the design and development of Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST).
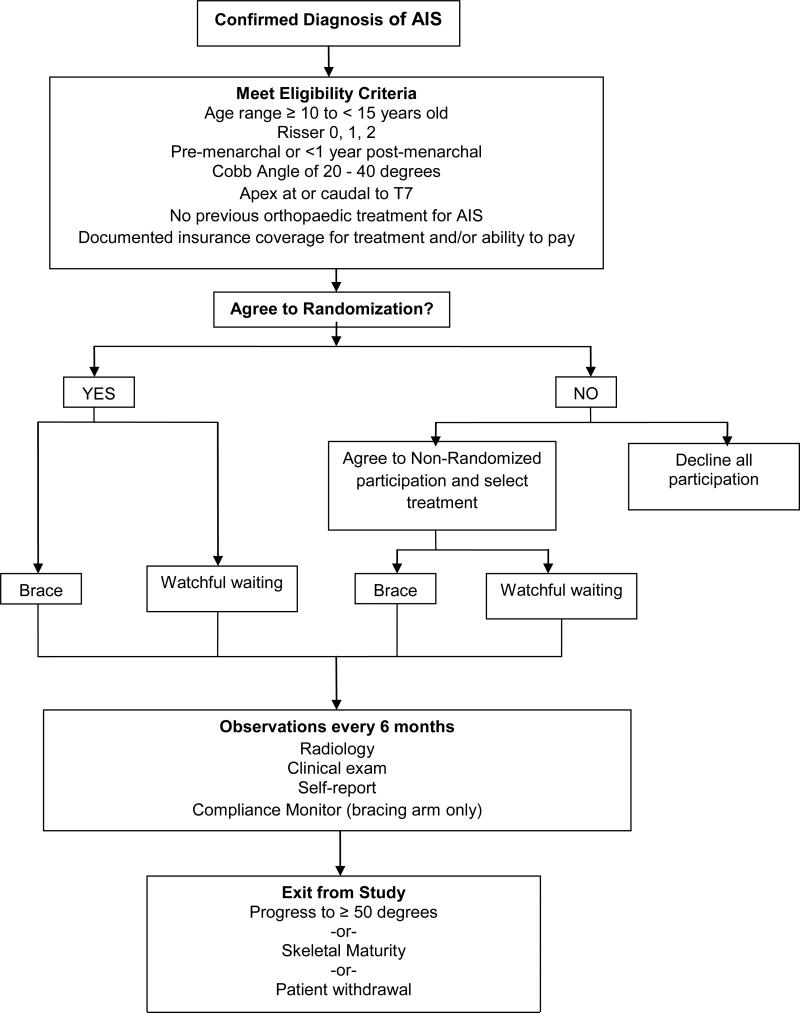
Summary of background data: Bracing has remained the standard of care for the nonoperative treatment of adolescent idiopathic scoliosis since the introduction of the Milwaukee brace in the late 1940s, but it has never been subjected to a rigorous evaluation of either its efficacy or its effectiveness. The BrAIST was designed to address the primary question: Do braces (specifically a thoracolumbosacral orthosis) lower the risk of curve progression to a surgical threshold (≥50°) in patients with adolescent idiopathic scoliosis relative to watchful waiting alone?
Methods: The authors describe the rationale for BrAIST, including the limitations of the current literature evaluating bracing for adolescent idiopathic scoliosis. Second, the authors describe the preliminary work, including the preparation of the National Institutes of Health clinical trials planning grant. Finally, the authors describe the trial design in detail.
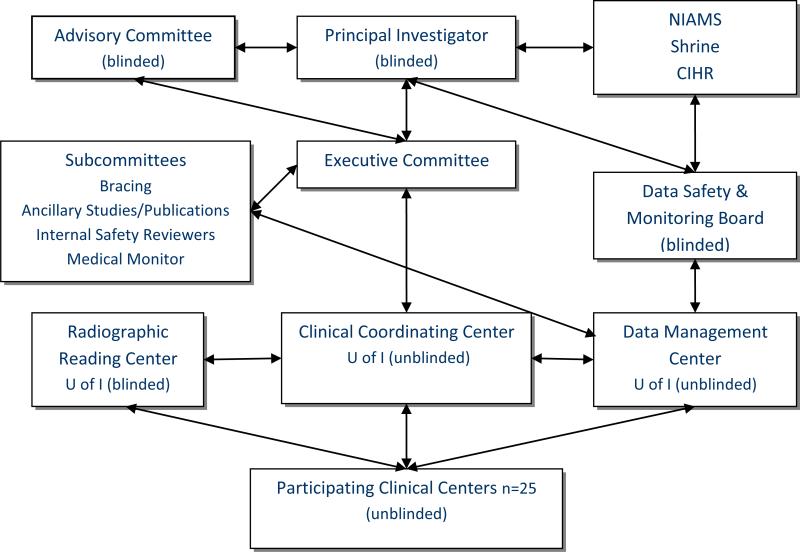
Results: BrAIST was conducted in 25 sites in North America. Subjects were treated either with a thoracolumbosacral orthosis or watchful waiting and followed every 6 months until they reached skeletal maturity or the surgical threshold of 50° Cobb angle.
Conclusion: Clinical decision making will be improved by translation of the BrAIST results into evidence-based prognosis and estimates of how the prognosis, specifically the risk of progressing to surgery, may be altered by the use of bracing.
Level of evidence: N/A.
Figures
References
-
- Nachemson AL, Lonstein JE, Weinstein SL. Scoliosis Research Society. Denver, Colorado: 1982. Report of the Prevalence and Natural History Committee of the Scoliosis Research Society.
-
- HCUP Kids’ Inpatient Database (KID) Healthcare Cost and Utilization Project (HCUP) Agency for Healthcare Research and Quality; Rockville, MD: 2009. www.hcup-us.ahrq.gov/kidoverview.jsp.
-
- Pehrsson K, Larsson S, Oden A, et al. Long-term follow-up of patients with untreated scoliosis. A study of mortality, causes of death, and symptoms. Spine. 1992;17:1091–6. - PubMed
-
- Weinstein SL, Dolan LA, Spratt KF, et al. Health and function of patients with untreated idiopathic scoliosis: a 50-year natural history study. JAMA. 2003;289:559–67. - PubMed
-
- Ascani E, Bartolozzi P, Logroscino CA, et al. Natural history of untreated idiopathic scoliosis after skeletal maturity. Symposium on Epidemiology, Natural History and Non-operative Treatment of Idiopathic Scoliosis. Spine. 1986;11:784–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
