

Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: a randomised trial
- PMID: 24026211
- PMCID: PMC3825495
- DOI: 10.1007/s00125-013-3039-1
Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: a randomised trial
Abstract
Aims/hypothesis: The aim of this work was to evaluate the efficacy and safety of canagliflozin vs placebo and sitagliptin in patients with type 2 diabetes who were being treated with background metformin.
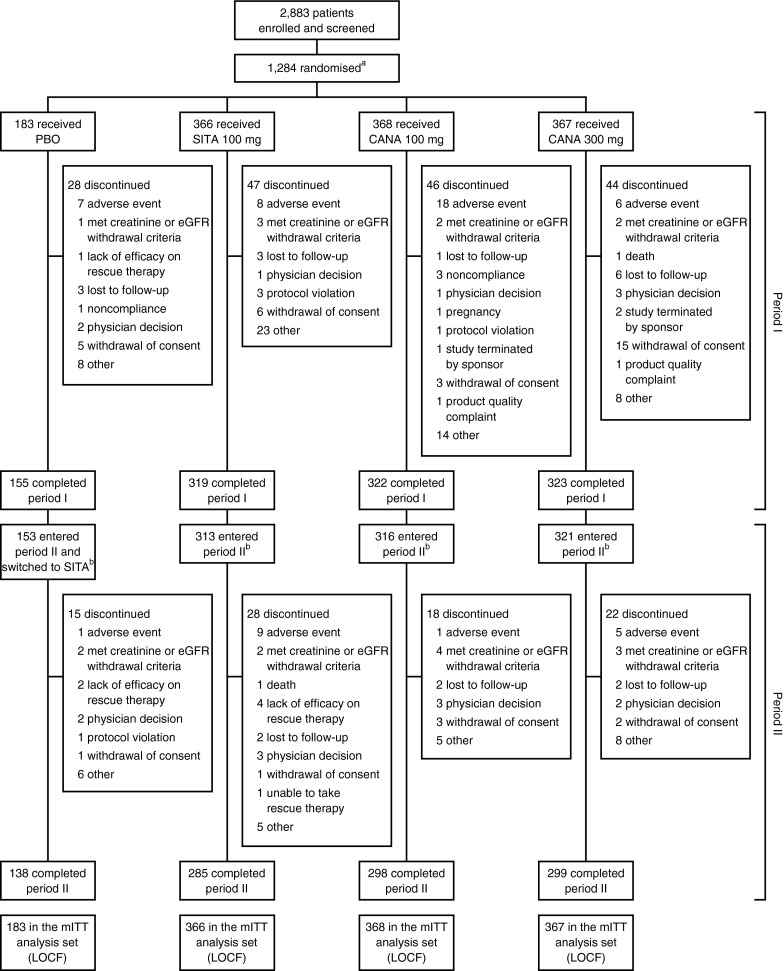
Methods: This randomised, double-blind, four-arm, parallel-group, Phase 3 study was conducted at 169 centres in 22 countries between April 2010 and August 2012. Participants (N = 1,284) with type 2 diabetes aged ≥ 18 and ≤ 80 years who had inadequate glycaemic control (HbA1c ≥ 7.0% [53 mmol/mol] and ≤10.5% [91 mmol/mol]) on metformin therapy received canagliflozin 100 mg or 300 mg, sitagliptin 100 mg, or placebo (n = 368, 367, 366, 183, respectively) for a 26 week, placebo- and active-controlled period followed by a 26 week, active-controlled period (placebo group switched to sitagliptin [placebo/sitagliptin]) and were included in the modified intent-to-treat analysis set. Randomisation was performed using a computer-generated schedule; participants, study centres and the sponsor were blinded to group assignment. The primary endpoint was change from baseline in HbA1c at week 26; secondary endpoints included changes in HbA1c (week 52) and fasting plasma glucose (FPG), body weight, and systolic blood pressure (BP; weeks 26 and 52). Adverse events (AEs) were recorded throughout the study.
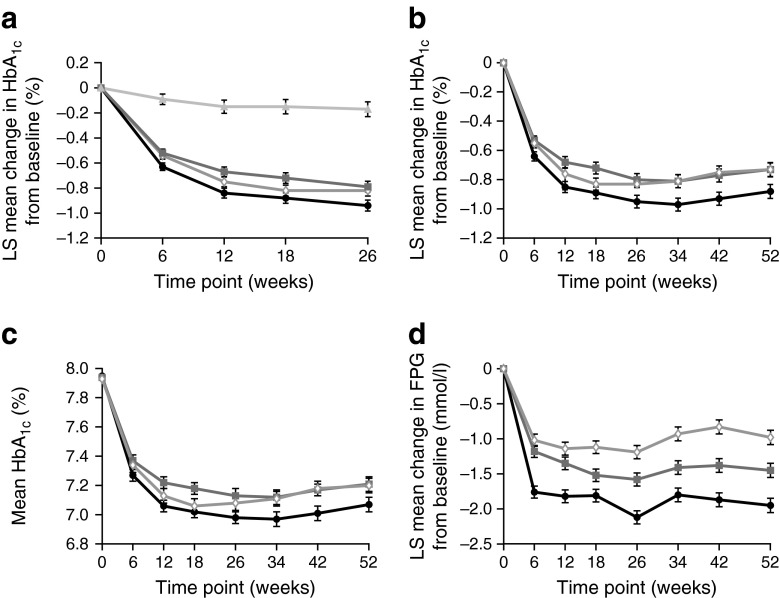
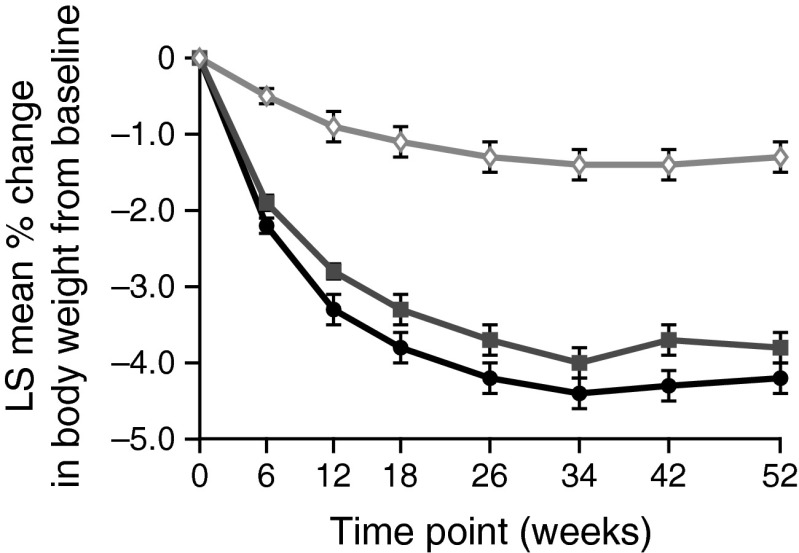
Results: At week 26, canagliflozin 100 mg and 300 mg reduced HbA1c vs placebo (-0.79%, -0.94%, -0.17%, respectively; p < 0.001). At week 52, canagliflozin 100 mg and 300 mg demonstrated non-inferiority, and canagliflozin 300 mg demonstrated statistical superiority, to sitagliptin in lowering HbA1c (-0.73%, -0.88%,-0.73%, respectively); differences (95% CI) vs sitagliptin were 0% (-0.12, 0.12) and -0.15% (-0.27, -0.03), respectively. Canagliflozin 100 mg and 300 mg reduced body weight vs placebo (week 26: -3.7%, -4.2%, -1.2%, respectively; p < 0.001) and sitagliptin (week 52: -3.8%, -4.2%, -1.3%, respectively; p < 0.001). Both canagliflozin doses reduced FPG and systolic BP vs placebo (week 26) and sitagliptin (week 52) (p < 0.001). Overall AE and AE-related discontinuation rates were generally similar across groups, but higher with canagliflozin 100 mg. Genital mycotic infection and osmotic diuresis-related AE rates were higher with canagliflozin; few led to discontinuations. Hypoglycaemia incidence was higher with canagliflozin.
Conclusions/interpretation: Canagliflozin improved glycaemia and reduced body weight vs placebo (week 26) and sitagliptin (week 52) and was generally well tolerated in patients with type 2 diabetes on metformin.
Clinical trial registry: ClinicalTrials.gov NCT01106677 FUNDING: This study was supported by Janssen Research & Development, LLC.
Figures
References
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia. 2012;55:1577–1596. doi: 10.1007/s00125-012-2534-0. - DOI - PubMed
-
- National Institute for Health and Clinical Excellence (2009) Type 2 diabetes: newer agents for blood glucose control in type 2 diabetes. NICE short clinical guideline 87. NICE, London - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
