

Diabetic autonomic neuropathy affects symptom generation and brain-gut axis
- PMID: 24026548
- PMCID: PMC3816908
- DOI: 10.2337/dc13-0347
Diabetic autonomic neuropathy affects symptom generation and brain-gut axis
Abstract
Objective: Long-term diabetes leads to severe peripheral, autonomous, and central neuropathy in combination with clinical gastrointestinal symptoms. The brain-gut axis thus expresses a neurophysiological profile, and heart rate variability (HRV) can be correlated with clinical gastrointestinal symptoms.
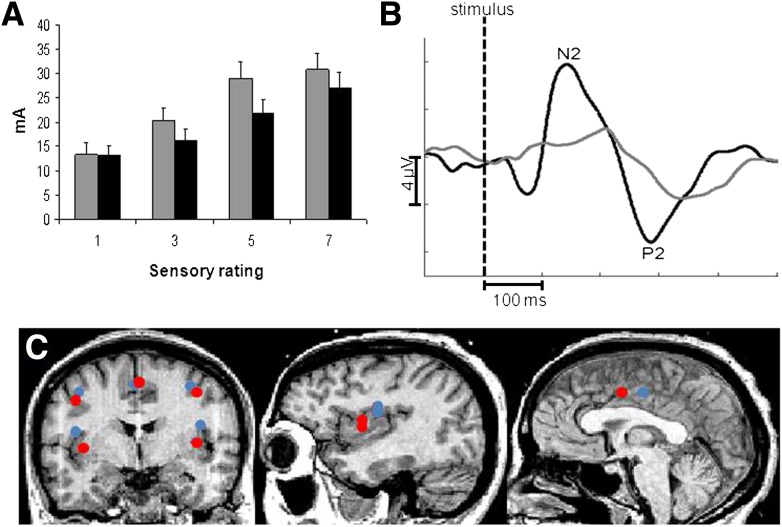
Research design and methods: Fifteen healthy volunteers and 15 diabetic patients (12 with type 1 diabetes) with severe gastrointestinal symptoms and clinical suspicion of autonomic neuropathy were included. Psychophysics and evoked brain potentials were assessed after painful rectosigmoid electrostimulations, and brain activity was modeled by brain electrical source analysis. Self-reported gastrointestinal symptoms (per the Patient Assessment of Upper Gastrointestinal Disorder Severity Symptom Index) and quality of life (SF-36 Short Form Survey) were collected.
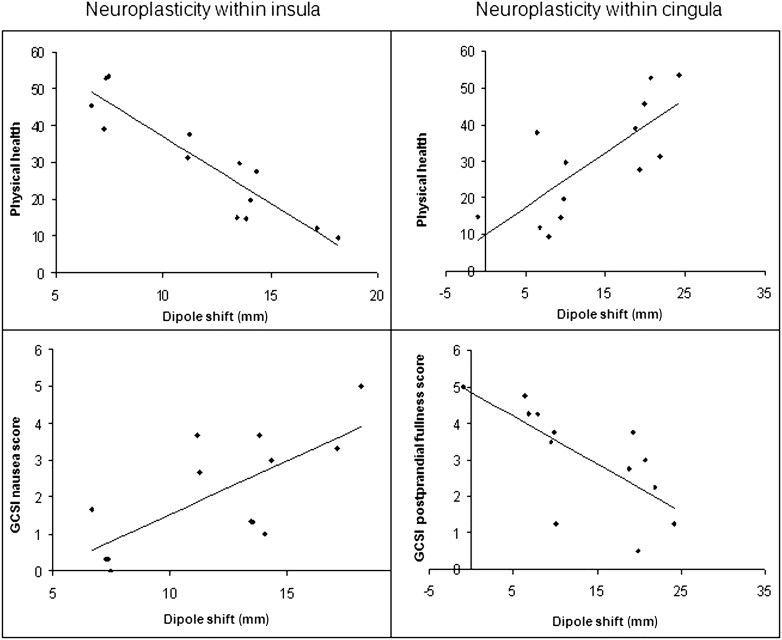
Results: Diabetic patients had autonomous neuropathy, evidenced by decreased electrocardiographic R-R interval (P = 0.03) and lower HRV (P = 0.008). Patients were less sensitive to painful stimulation (P = 0.007), had prolonged latencies of evoked potentials (P ≤ 0.001), and showed diminished amplitude of the N2-P2 component in evoked potentials (P = 0.01). There was a caudoanterior shift of the insular brain source (P = 0.01) and an anterior shift of the cingulate generator (P = 0.01). Insular source location was associated with HRV assessments (all P < 0.02), and the shift (expressed in mm) correlated negatively with physical health (P < 0.001) and positively with nausea (P = 0.03) and postprandial fullness (P = 0.03). Cingulate source shift was correlated negatively with physical health (P = 0.005) and positively with postprandial fullness (P ≤ 0.001).
Conclusions: This study provides evidence for interaction between autonomic neuropathy and peripheral nervous degeneration, as well as changes in dipole sources in diabetic patients with gastrointestinal symptoms. The findings may lead to improved treatment modalities targeting pharmacological neuroprotection or neuromodulation.
Figures
References
-
- Kahn R. Proceedings of a consensus development conference on standardized measures in diabetic neuropathy. Autonomic nervous system testing. Diabetes Care 1992;15:1095–1103. - PubMed
-
- Bytzer P, Talley NJ, Leemon M, Young LJ, Jones MP, Horowitz M. Prevalence of gastrointestinal symptoms associated with diabetes mellitus: a population-based survey of 15,000 adults. Arch Intern Med 2001;161:1989–1996 - PubMed
-
- Holst JJ, Gromada J. Role of incretin hormones in the regulation of insulin secretion in diabetic and nondiabetic humans. Am J Physiol Endocrinol Metab 2004;287:E199–E206 - PubMed
-
- Orskov C, Holst JJ, Nielsen OV. Effect of truncated glucagon-like peptide-1 [proglucagon-(78-107) amide] on endocrine secretion from pig pancreas, antrum, and nonantral stomach. Endocrinology 1988;123:2009–2013 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
