

The use of (18)F-FDG-PET/CT for diagnosis and treatment monitoring of inflammatory and infectious diseases
- PMID: 24027590
- PMCID: PMC3763592
- DOI: 10.1155/2013/623036
The use of (18)F-FDG-PET/CT for diagnosis and treatment monitoring of inflammatory and infectious diseases
Abstract
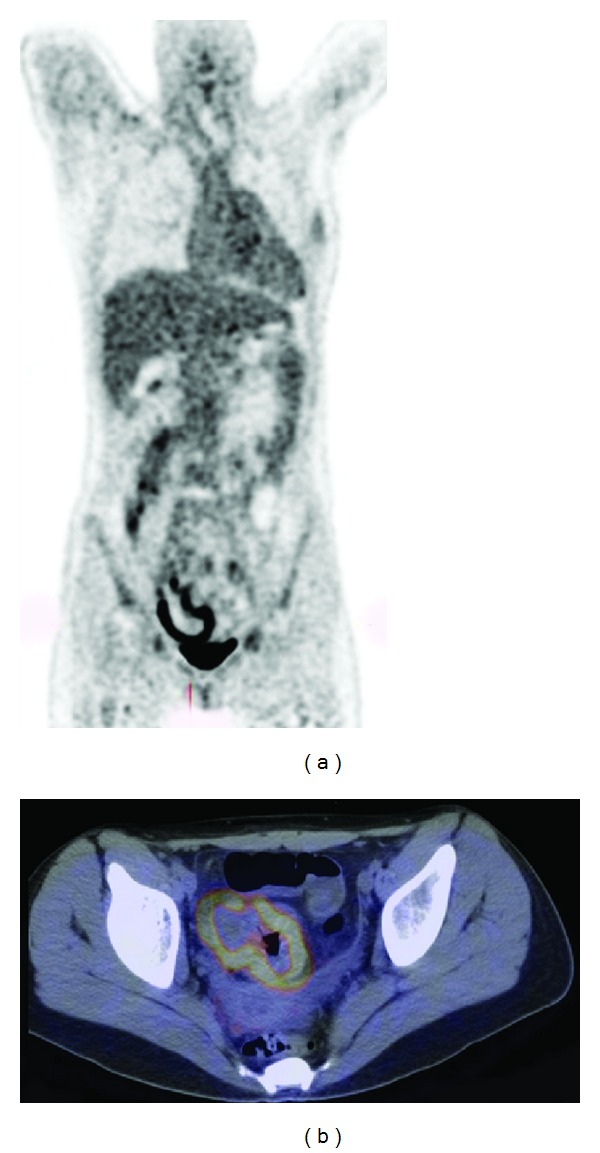
FDG-PET, combined with CT, is nowadays getting more and more relevant for the diagnosis of several infectious and inflammatory diseases and particularly for therapy monitoring. Thus, this paper gives special attention to the role of FDG-PET/CT in the diagnosis and therapy monitoring of infectious and inflammatory diseases. Enough evidence in the literature already exists about the usefulness of FDG-PET/CT in the diagnosis, management, and followup of patients with sarcoidosis, spondylodiscitis, and vasculitis. For other diseases, such as inflammatory bowel diseases, rheumatoid arthritis, autoimmune pancreatitis, and fungal infections, hard evidence is lacking, but studies also point out that FDG-PET/CT could be useful. It is of invaluable importance to have large prospective multicenter studies in this field to provide clear answers, not only for the status of nuclear medicine in general but also to reduce high costs of treatment.
Figures





References
-
- Ruf J, Oeser C, Amthauer H. Clinical role of anti-granulocyte MoAb versus radiolabeled white blood cells. Quarterly Journal of Nuclear Medicine and Molecular Imaging. 2010;54(6):599–616. - PubMed
-
- Signore A, Glaudemans AWJM. The molecular imaging approach to image infections and inflammation by nuclear medicine techniques. Annals of Nuclear Medicine. 2011;25(10):681–700. - PubMed
-
- Arend WP, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis and Rheumatism. 1990;33(8):1129–1134. - PubMed
-
- Hunder GG, Bloch DA, Michel BA, et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis and Rheumatism. 1990;33(8):1122–1128. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
