

Postoperative pain and perioperative outcomes after laparoscopic radical hysterectomy and abdominal radical hysterectomy in patients with early cervical cancer: a randomised controlled trial
- PMID: 24028441
- PMCID: PMC3856515
- DOI: 10.1186/1745-6215-14-293
Postoperative pain and perioperative outcomes after laparoscopic radical hysterectomy and abdominal radical hysterectomy in patients with early cervical cancer: a randomised controlled trial
Abstract
Background: Non-randomised studies have suggested that the postoperative complications of (Campos LS, Limberger LF, Stein AT, Kalil AN) laparoscopic radical hysterectomy are similar to those in abdominal radical hysterectomy. However, no study evaluating postoperative pain comparing both techniques has been published thus far. Our objective was to compare pain intensity and other perioperative outcomes between laparoscopic radical hysterectomy (LRH) and abdominal radical hysterectomy (ARH) in early cervical cancer.
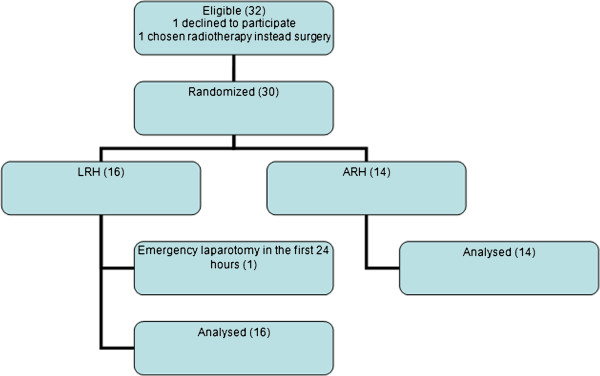
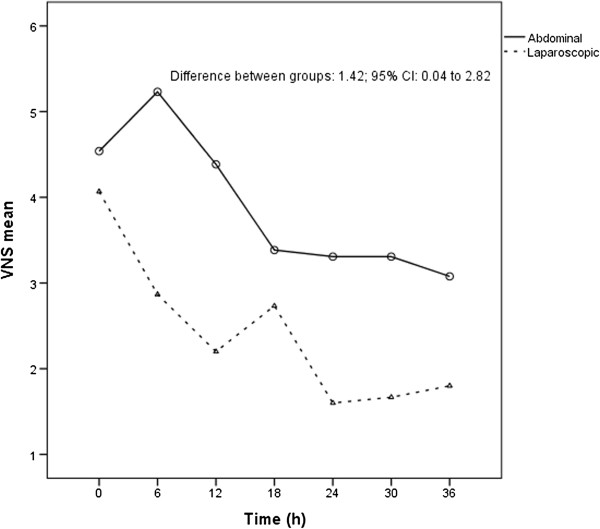
Methods: This single centre, randomised, controlled trial enrolled 30 cervical cancer patients who were clinically staged IA2 with lymph vascular invasion and IB according to the FIGO (International Federation of Gynaecology and Obstetrics) classification, and underwent LRH or ARH between late 1999 and early 2004. Postoperative pain, as measured by a 10-point numerical rate scale, was considered the primary endpoint. Postoperative pain was assessed every six hours during a patient's usual postoperative care. Perioperative outcomes were also registered. Both surgical techniques were executed by the same surgical team. Secondary outcomes included intraoperative and other postoperative surgicopathological factors and 5-year survival rates.
Results: IA2 patients with lymphatic vascular space invasion and IB cervical cancer patients were randomised to either the LRH group (16 patients) or the ARH group (14 patients). Four patients (25%) in the LRH group and 5 patients (36%) in the ARH group presented with transoperative or serious postoperative complications. All of the transoperative complications occurred in the LRH group. The relative risk of presenting with complications was 0.70; CI 95% (0.23-2.11); P = 0.694. LRH group mean pain score was significantly lower than ARH after 36 h of observation (P = 0.044; mean difference score: 1.42; 95% CI: 0.04-2.80). The survival results will be published elsewhere.
Conclusions: LRH provided lower pain scores after 36 h of observation in this series. The perioperative and serious postoperative complications ratios were comparable between the groups.
Trial registration: NCT01258413.
Figures
References
-
- Instituto Nacional do Câncer. Estimativas da Incidência e Mortalidade por Câncer. Rio de Janeiro, Brazil: INCA, National Institute of Cancer; 2006.
-
- Benedet JL, Ngam HYS, Hacker NF. FIGO Committee on Gynecologic Oncology: Staging Classifications and Clinical Practice Guidelines of Gynaecologic Cancer. 2010. [ http://www.figo.org] - PubMed
-
- Ramirez PT, Soliman PT, Schmeler KM, dos Reis R, Frumovitz M. Laparoscopic and robotic techniques for radical hysterectomy in patients with early-stage cervical cancer. Gynecol Oncol. 2008;110(Suppl 2):21–24. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
