

Androgen deficiency in male patients diagnosed with ANCA-associated vasculitis: a cause of fatigue and reduced health-related quality of life?
- PMID: 24028544
- PMCID: PMC3979147
- DOI: 10.1186/ar4297
Androgen deficiency in male patients diagnosed with ANCA-associated vasculitis: a cause of fatigue and reduced health-related quality of life?
Abstract
Introduction: Low testosterone levels in men are associated with fatigue, limited physical performance and reduced health-related quality of life (HRQOL); however, this relationship has never been assessed in patients with anti-neutrophil cytoplasmic antibodies (ANCA) -associated vasculitides (AAV). The aim of this study was to assess the prevalence of androgen deficiency and to investigate the role of testosterone in fatigue, limited physical condition and reduced HRQOL in men with AAV.
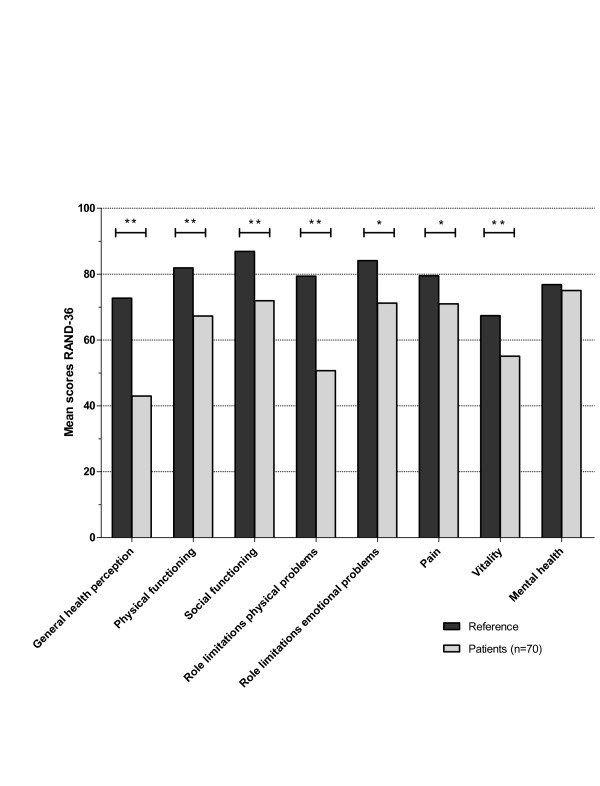
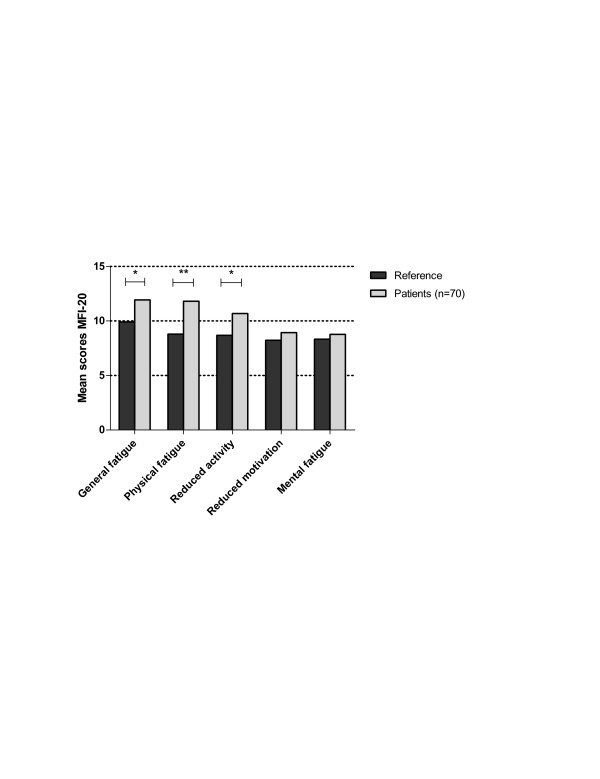
Methods: Male patients with AAV in remission were included in this study. Fatigue and HRQOL were assessed by the multi-dimensional fatigue inventory (MFI)-20 and RAND-36 questionnaires.
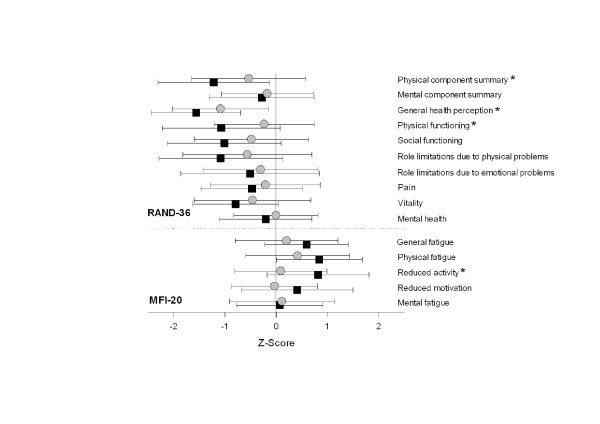
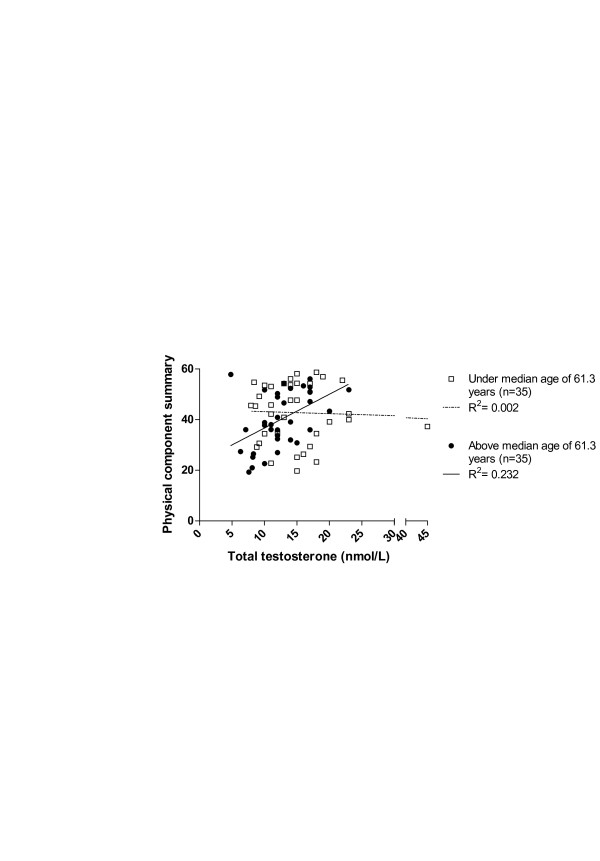
Results: Seventy male patients with a mean age of 59 years (SD 12) were included. Scores of almost all subscales of both questionnaires were significantly worse in patients compared to controls. Mean total testosterone and free testosterone levels were 13.8 nmol/L (SD 5.6) and 256 pmol/L (SD 102), respectively. Androgen deficiency (defined according to Endocrine Society Clinical Practice Guidelines) was present in 47% of patients. Scores in the subscales of general health perception, physical functioning and reduced activity were significantly worse in patients with androgen deficiency compared to patients with normal androgen levels. Testosterone and age were predictors for the RAND-36 physical component summary in multiple linear regression analysis. Testosterone, age, vasculitis damage index (VDI) and C-reactive protein (CRP) were associated with the MFI-20 subscale of general fatigue.
Conclusions: This study showed that androgen deficiency was present in a substantial number of patients with AAV. Testosterone was one of the predictors for physical functioning and fatigue. Testosterone may play a role in fatigue, reduced physical performance and HRQOL in male patients with AAV.
Figures

References
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;15:1–11. - PubMed
-
- Mukhtyar C, Flossmann O, Hellmich B, Bacon P, Cid M, Cohen-Tervaert JW, Gross WL, Guillevin L, Jayne D, Mahr A, Merkel PA, Raspe H, Scott D, Witter J, Yazici H, Luqmani RA. European Vasculitis Study Group (EUVAS) Outcomes from studies of antineutrophil cytoplasm antibody associated vasculitis: a systematic review by the European League Against Rheumatism systemic vasculitis task force. Ann Rheum Dis. 2008;15:1004–1010. - PubMed
-
- Hoffman GS, Drucker Y, Cotch MF, Locker GA, Easley K, Kwoh K. Wegener's granulomatosis: patient-reported effects of disease on health, function, and income. Arthritis Rheum. 1998;15:2257–2262. - PubMed
-
- Reinhold-Keller E, Herlyn K, Wagner-Bastmeyer R, Gutfleisch J, Peter HH, Raspe HH, Gross WL. Effect of Wegener's granulomatosis on work disability, need for medical care, and quality of life in patients younger than 40 years at diagnosis. Arthritis Rheum. 2002;15:320–325. - PubMed
-
- Koutantji M, Harrold E, Lane SE, Pearce S, Watts RA, Scott DG. Investigation of quality of life, mood, pain, disability, and disease status in primary systemic vasculitis. Arthritis Rheum. 2003;15:826–837. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
