

An evaluation of emergency medical services stroke protocols and scene times
- PMID: 24028711
- PMCID: PMC3973028
- DOI: 10.3109/10903127.2013.825354
An evaluation of emergency medical services stroke protocols and scene times
Abstract
Background: Acute stroke patients require immediate medical attention. Therefore, American Stroke Association guidelines recommend that for suspected stroke cases, emergency medical services (EMS) personnel spend less than 15 minutes on-scene at least 90% of the time. However, not all EMS providers include specific scene time limits in their stroke patient care protocols.
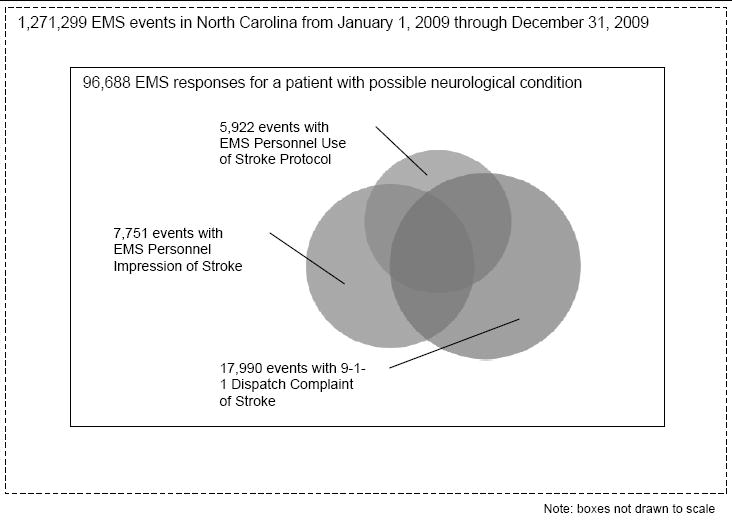
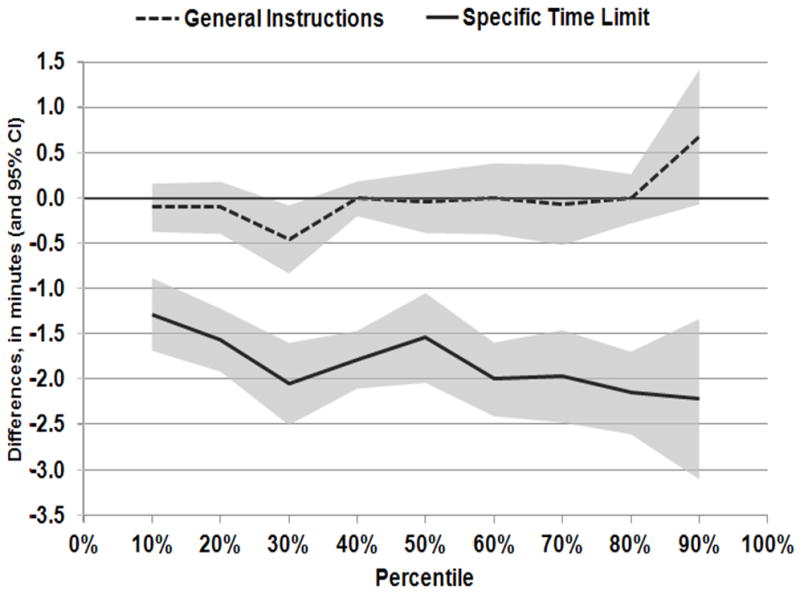
Objective: We sought to determine whether having a protocol with a specific scene time limit was associated with less time EMS spent on scene. Methods. Stroke protocols from the 100 EMS systems in North Carolina were collected and abstracted for scene time instructions. Suspected stroke events occurring in 2009 were analyzed using data from the North Carolina Prehospital Medical Information System. Scene time was defined as the time from EMS arrival at the scene to departure with the patient. Quantile regression was used to estimate how the 90th percentile of the scene time distribution varied by systems with protocol instructions limiting scene time, adjusting for system patient volume and metropolitan status.
Results: In 2009, 23 EMS systems in North Carolina had no instructions regarding scene time; 73 had general instructions to minimize scene time; and 4 had a specific limit for scene time (i.e., 10 or 15 min). Among 9,723 eligible suspected stroke events, mean scene time was 15.9 minutes (standard deviation 6.9 min) and median scene time was 15.0 minutes (90th percentile 24.3 min). In adjusted quantile regression models, the estimated reduction in the 90th percentile scene time, comparing protocols with a specific time limit to no instructions, was 2.2 minutes (95% confidence interval 1.3, 3.1 min). The difference in 90th percentile scene time between general and absent instructions was not statistically different (0.7 min [95% confidence interval -0.1, 1.4 min]).
Conclusion: Protocols with specific scene time limits were associated with EMS crews spending less time at the scene while general instructions were not. These findings suggest EMS systems can modestly improve scene times for stroke by specifying a time limit in their protocols.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Saver JL. Time is brain—quantified. Stroke. 2006;37(1):263–266. - PubMed
-
- Jauch EC, Saver JL, Adams HP, Bruno A, Connors JJ, Demaerschalk BM, Khatri P, McMullan PW, Qureshi AI, Rosenfield K, Scott PA, Summers DR, Wang DZ, Wintermark M, Yonas H. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(3):870–947. - PubMed
-
- Kothari R, Jauch E, Broderick J, Brott T, Sauerbeck L, Khoury J, Liu T. Acute stroke: Delays to presentation and emergency department evaluation. Ann Emerg Med. 1999;33:3–8. - PubMed
-
- Morris DL, Rosamond W, Madden K, Schultz C, Hamilton S. Prehospital and emergency department delays after acute stroke: The Genentech stroke presentation survey. Stroke. 2000;31(11):2585–2590. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical