

Practice Guideline
doi: 10.6004/jnccn.2013.0127.
Acute myeloid leukemia, version 2.2013
Affiliations
- PMID: 24029121
- PMCID: PMC4161234
- DOI: 10.6004/jnccn.2013.0127
Item in Clipboard
Practice Guideline
Acute myeloid leukemia, version 2.2013
J Natl Compr Canc Netw.
.
Abstract
These NCCN Guidelines Insights summarize several key updates to the NCCN Guidelines for Acute Myeloid Leukemia and discuss the clinical evidence that support the recommendations. The updates described in this article focus on the acute promyelocytic leukemia (APL) section, featuring recommendations for additional induction/consolidation regimens in patients with low- or intermediate-risk APL, and providing guidance on maintenance strategies for APL.
Conflict of interest statement
The NCCN Guidelines Staff have no conflicts to disclose.
Figures
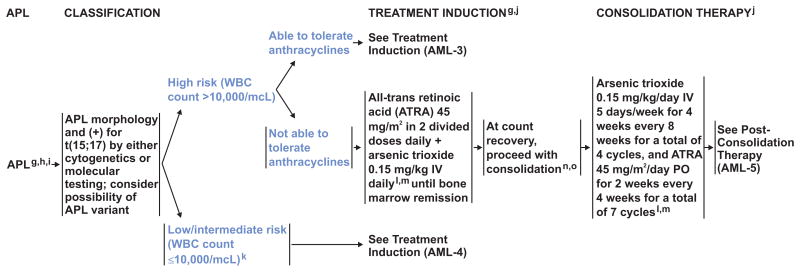
gSeveral groups have published large trials with excellent outcomes. However, to achieve the expected results, one needs to use the regimen consistently through all components and not mix induction from one trial with consolidation from another. hTherapy-related APL is treated the same as de novo APL. i In patients with clinical and pathologic features of APL, start ATRA upon first suspicion of APL without waiting for genetic confirmation of the diagnosis. Early initiation of ATRA may prevent the lethal complication of bleeding. If cytogenetic and molecular testing do not confirm APL, discontinue ATRA and continue treatment as for AML. jMonitor for APL differentiation syndrome and coagulopathy; see Supportive Care (AML-C 2 of 2). kNew data suggest similar outcomes in patients with low or intermediate risk. lShen ZX, Shi ZZ, Fang J, et al. All-trans retinoic acid/As2O3 combination yields a high quality remission and survival in newly diagnosed acute promyelocytic leukemia. Proc Natl Acad Sci USA 2004;101(15):5328-35. Ravandi F, Estey E, Jones D, et al. Effective treatment of acute promyelocytic leukemia with all-trans-retinoic acid, arsenic trioxide, and gemtuzumab ozogamicin. J Clin Oncol 2009;27:504-510. mSee Arsenic trioxide monitoring, Supportive Care (AML-C 2 of 2). nPremature morphologic and molecular assessment (day 10-14 marrow) can be misleading; a nadir marrow is not recommended. Patients often remain molecularly positive at the end of induction, even when the marrow shows morphologic remission. The first assessment of molecular remission should be made after consolidation. oEarly mortality is related to bleeding, differentiation syndrome, or infection. Persistent disease is rare. See first relapse on AML-6.
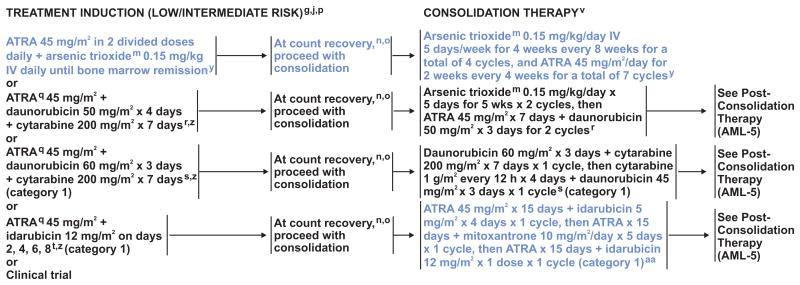
gSeveral groups have published large trials with excellent outcomes. However, to achieve the expected results, one needs to use the regimen consistently through all components and not mix induction from one trial with consolidation from another. j Monitor for APL differentiation syndrome and coagulopathy; see Supportive Care (AML-C 2 of 2). mSee Arsenic trioxide monitoring, Supportive Care (AML-C 2 of 2). nPremature morphologic and molecular assessment (day 10-14 marrow) can be misleading; a nadir marrow is not recommended. Patients often remain molecularly positive at the end of induction, even when the marrow shows morphologic remission. The first assessment of molecular remission should be made after consolidation. oEarly mortality is related to bleeding, differentiation syndrome, or infection. Persistent disease is rare. See first relapse on AML-6. pFor patients with (or who develop) a high WBC count (>10,000), consider prophylactic dexamethasone to prevent differentiation syndrome. qData suggest that lower doses of ATRA (25 mg/m2) may be used in adolescents. rPowell BL, Moser B, Stock W, et al. Arsenic trioxide improves event-free and overall survival for adults with acute promyelocytic leukemia: North American Leukemia Intergroup Study C9710. Blood 2010;116:3751-3757. sAdes LA, Sanz MA, Chevret S, et al. Treatment of newly diagnosed acute promyelocytic leukemia (APL): A comparison of French-Belgian-Swiss and PETHEMA results. Blood 2008;111:1078-1086. tSanz MA, Montesinos P, Rayon C, et al. Risk-adapted treatment of acute promyelocytic leukemia based on all trans retinoic acid and anthracycline with addition of cytarabine in consolidation therapy for high risk patients: further improvements in treatment outcomes. Blood 2010;115:5137-5146. vAll regimens include high cumulative doses of cardiotoxic agents. Cardiac function should be assessed prior to each anthracycline/mitoxantrone-containing course. yLo-Coco F, Avvisati G, Orlando SM, et al. ATRA and arsenic trioxide (ATO) versus ATRA and idarubicin (AIDA) for newly diagnosed, non high-risk acute promyelocytic leukemia (APL): results of the phase III, prospective, randomized, intergroup APL0406 study by the Italian-German Cooperative Groups Gimema-SAL-AMLSG [abstract.] Blood 2012;120:Abstract 6. zFor patients who have rapidly escalating WBC counts or other high-risk features during course of induction therapy, see Consolidation Therapy on AML-3. aaLo-Coco F, Avvisati G, Vignetti M, et al. Front-line treatment of acute promyelocytic leukemia with AIDA induction followed by risk-adapted consolidation for adult patients younger than 61 years: results of the AIDA-2000 trial of the GIMEMA Group. Blood 2010;116:3171-3179.
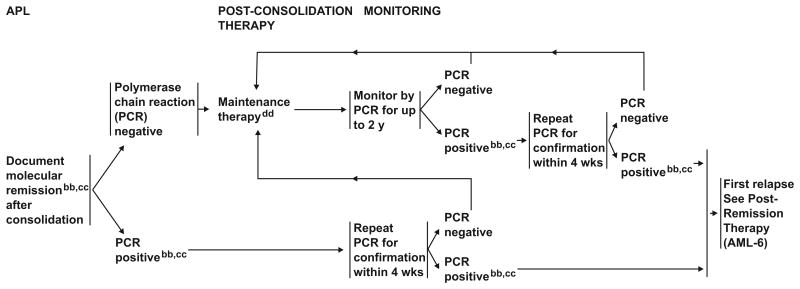
bbPCR should be performed on a marrow sample at completion of consolidation to document molecular remission. Subsequent monitoring by PCR can be done with peripheral blood, although marrow is a more sensitive monitoring technique and may give earlier signs of relapse. Prior practice guidelines have recommended monitoring marrow by PCR every 3 mo for 2 y to detect molecular relapse. We continue to endorse this for high-risk patients, those >age 60 y or who had long interruptions during consolidation, or patients not able to tolerate maintenance. Clinical experience indicates that risk of relapse in patients with low-risk disease who are in molecular remission at completion of consolidation is low and monitoring may not be necessary outside the setting of a clinical trial. ccTo confirm PCR positivity, a second marrow sample should be done in 2-4 weeks in a reliable laboratory. If molecular relapse is confirmed by a second positive test, treat as first relapse (AML-6).If the second test was negative, frequent monitoring (every 3 mo for 2 y) is strongly recommended to confirm that the patient remains negative. The PCR testing lab should indicate level of sensitivity of assay for positivity (most clinical labs have a sensitivity level of 10-4), and testing should be done in the same lab to maintain the same level of sensitivity. Consider consultation with a physician experienced in molecular diagnostics if results are equivocal. ddThe majority of studies showing benefit with maintenance occurred prior to the use of ATRA and/or arsenic trioxide and/or cytarabine for consolidation. Maintenance therapy should follow the initial treatment protocol. The role of maintenance chemotherapy remains unclear, particularly for patients with low-risk disease who achieve a molecular remission at the end of consolidation. Avvisati G, Lo-Coco F, Paoloni FP, et al. AIDA 0493 protocol for newly diagnosed acute promyelocytic leukemia: very long-term results and role of maintenance. Blood 2011;117:4716-4725.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- National Cancer Institute. SEER Stat Fact Sheets: Acute Myeloid Leukemia. Bethesda, MD: 2013. [Accessed May 7, 2013]. Available at: http://seer.cancer.gov/statfacts/html/amyl.html.
-
- Arber DA, Vardiman JW, Brunning RD, et al. Acute myeloid leukemia with recurrent genetic abnormalities. In: Swerdlow SH, Campo E, Harris NL, et al., editors. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th. Lyon, France: IARC; 2008. pp. 110–123.
-
- Powell BL. Arsenic trioxide in acute promyelocytic leukemia: potion not poison. Expert Rev Anticancer Ther. 2011;11:1317–1319. - PubMed
-
- Tallman MS, Altman JK. Curative strategies in acute promyelocytic leukemia. Hematology Am Soc Hematol Educ Program. 2008:391–399. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
