

Patching the heart: cardiac repair from within and outside
- PMID: 24030022
- PMCID: PMC3886802
- DOI: 10.1161/CIRCRESAHA.113.300216
Patching the heart: cardiac repair from within and outside
Abstract
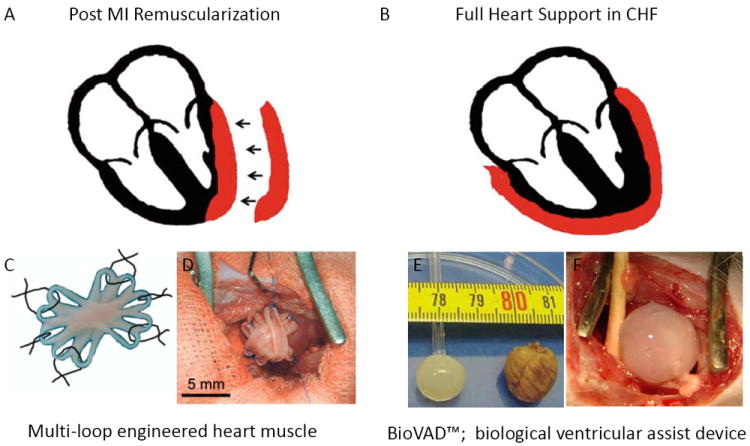
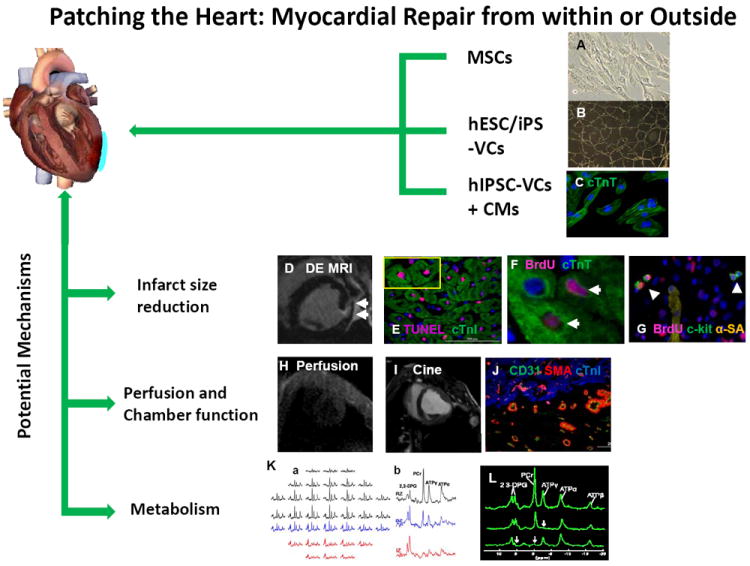
Transplantation of engineered tissue patches containing either progenitor cells or cardiomyocytes for cardiac repair is emerging as an exciting treatment option for patients with postinfarction left ventricular remodeling. The beneficial effects may evolve directly from remuscularization or indirectly through paracrine mechanisms that mobilize and activate endogenous progenitor cells to promote neovascularization and remuscularization, inhibit apoptosis, and attenuate left ventricular dilatation and disease progression. Despite encouraging results, further improvements are necessary to enhance current tissue engineering concepts and techniques and to achieve clinical impact. Herein, we review several strategies for cardiac remuscularization and paracrine support that can induce cardiac repair and attenuate left ventricular dysfunction from both within and outside the myocardium.
Keywords: heart failure; paracrine; tissue engineering; tissue therapy.
Figures
References
-
- McMurray JJ, Pfeffer MA. Heart failure. Lancet. 2005;365:1877–1889. - PubMed
-
- Orlic D, Kajstura J, Chimenti S, Jakoniuk I, Anderson SM, Li B, Pickel J, McKay R, Nadal-Ginard B, Bodine DM, Leri A, Anversa P. Bone marrow cells regenerate infarcted myocardium. Nature. 2001;410:701–705. - PubMed
-
- Beltrami AP, Barlucchi L, Torella D, Baker M, Limana F, Chimenti S, Kasahara H, Rota M, Musso E, Urbanek K, Leri A, Kajstura J, Nadal-Ginard B, Anversa P. Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell. 2003;114:763–776. - PubMed
-
- Muller-Ehmsen J, Whittaker P, Kloner RA, Dow JS, Sakoda T, Long TI, Laird PW, Kedes L. Survival and development of neonatal rat cardiomyocytes transplanted into adult myocardium. Journal of molecular and cellular cardiology. 2002;34:107–116. - PubMed
-
- Murry CE, Whitney ML, Laflamme MA, Reinecke H, Field LJ. Cellular therapies for myocardial infarct repair. Cold Spring Harb Symp Quant Biol. 2002;67:519–526. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
