

Effects of quality improvement in health facilities and community mobilization through women's groups on maternal, neonatal and perinatal mortality in three districts of Malawi: MaiKhanda, a cluster randomized controlled effectiveness trial
- PMID: 24030269
- PMCID: PMC5102328
- DOI: 10.1093/inthealth/iht011
Effects of quality improvement in health facilities and community mobilization through women's groups on maternal, neonatal and perinatal mortality in three districts of Malawi: MaiKhanda, a cluster randomized controlled effectiveness trial
Abstract
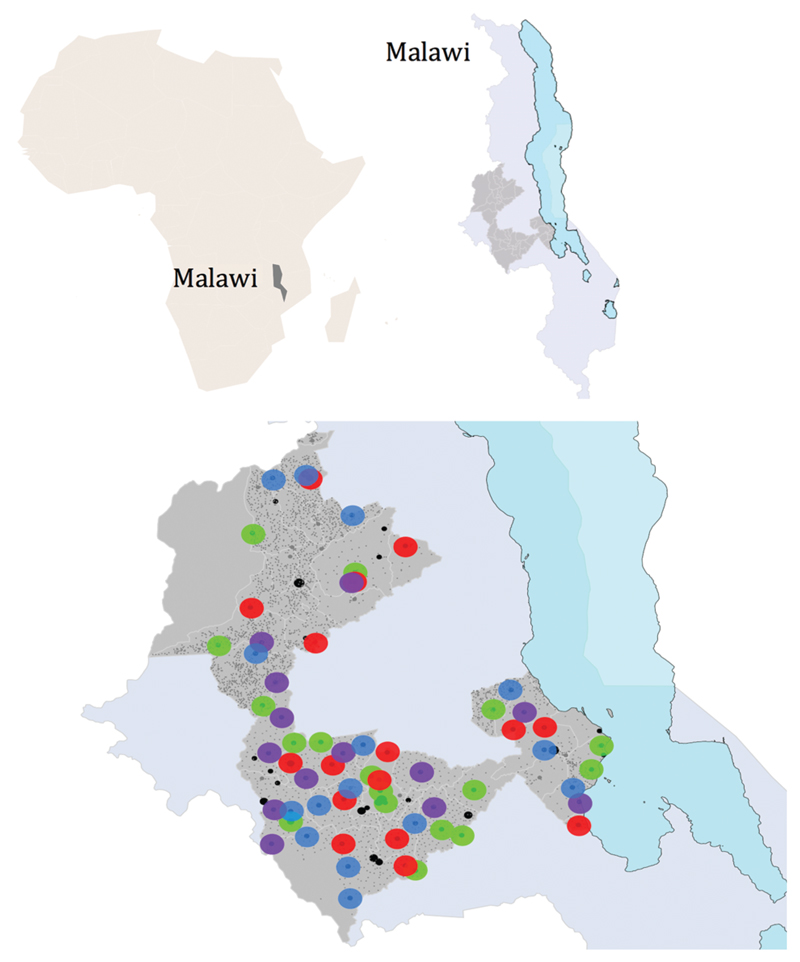
Background: Maternal, perinatal and neonatal mortality remains high in low-income countries. We evaluated community and facility-based interventions to reduce deaths in three districts of Malawi.
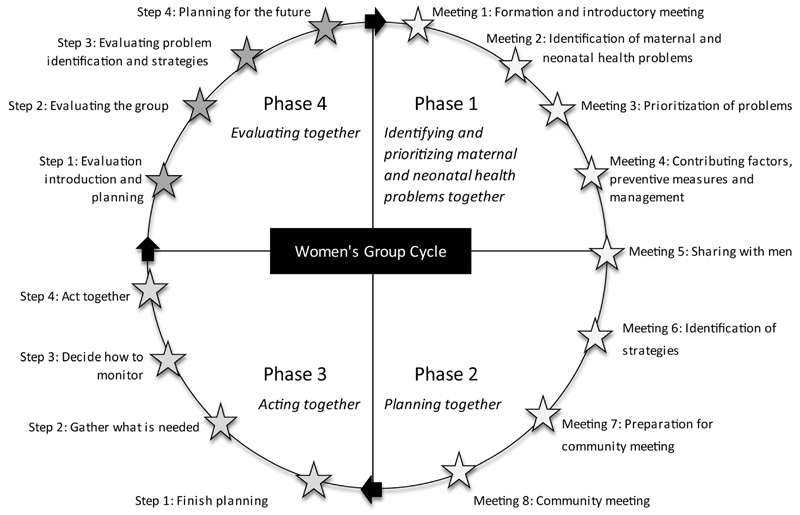
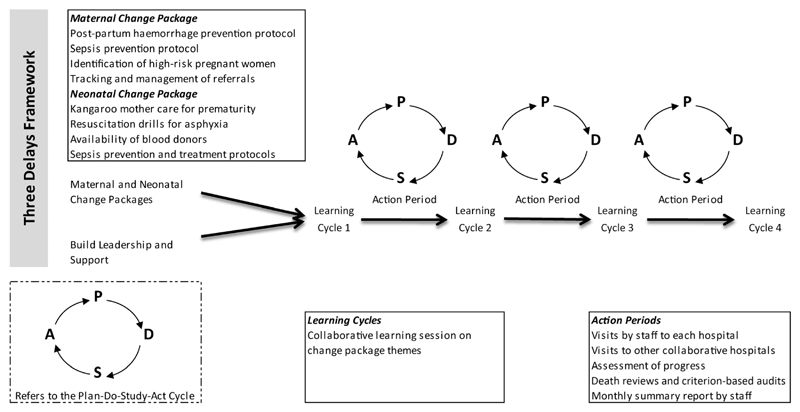
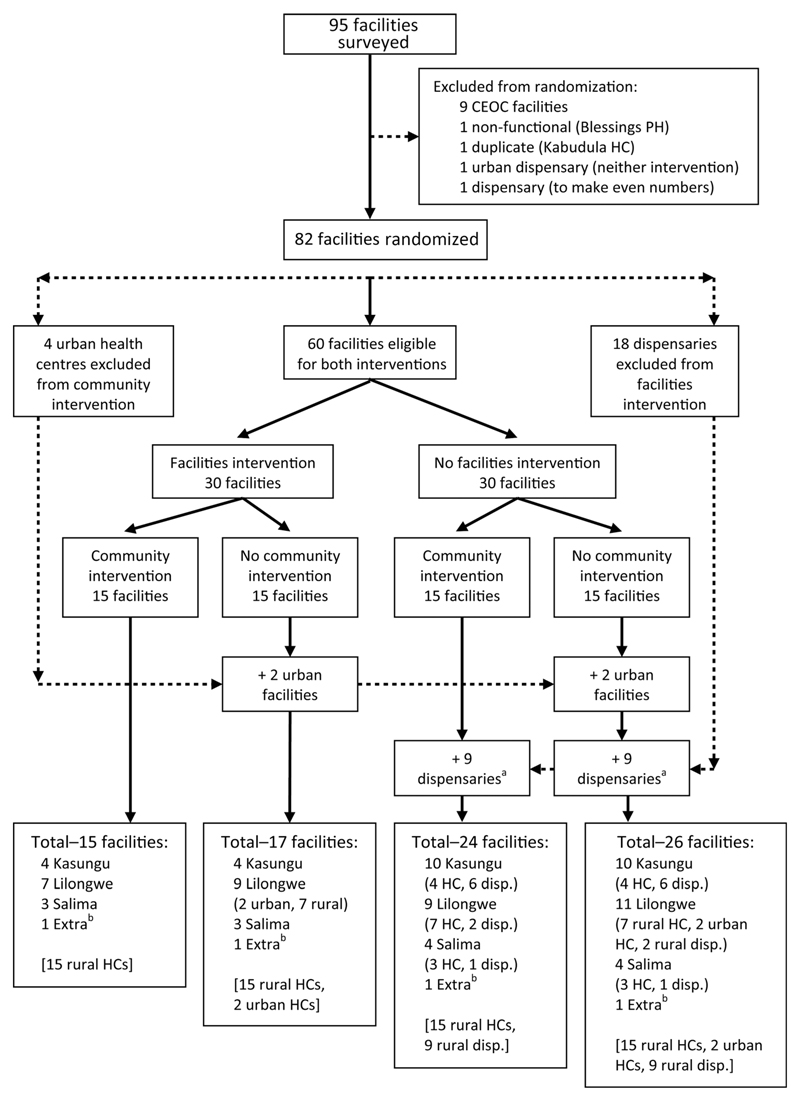
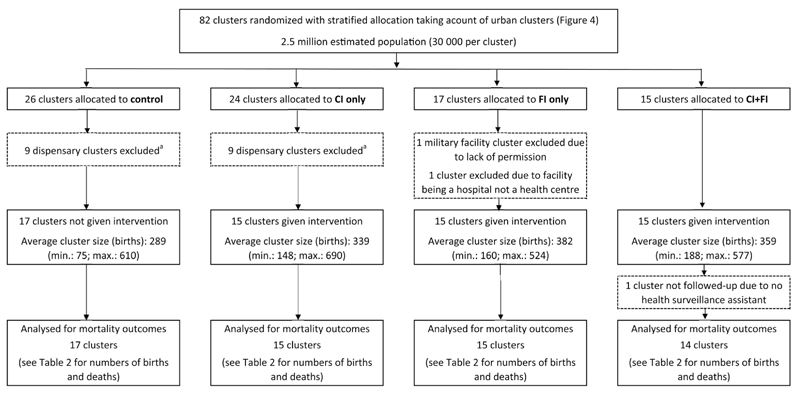
Methods: We evaluated a rural participatory women's group community intervention (CI) and a quality improvement intervention at health centres (FI) via a two-by-two factorial cluster randomized controlled trial. Consenting pregnant women were followed-up to 2 months after birth using key informants. Primary outcomes were maternal, perinatal and neonatal mortality. Clusters were health centre catchment areas assigned using stratified computer-generated randomization. Following exclusions, including non-birthing facilities, 61 clusters were analysed: control (17 clusters, 4912 births), FI (15, 5335), CI (15, 5080) and FI + CI (14, 5249). This trial was registered as International Standard Randomised Controlled Trial [ISRCTN18073903]. Outcomes for 14,576 and 20,576 births were recorded during baseline (June 2007-September 2008) and intervention (October 2008-December 2010) periods.
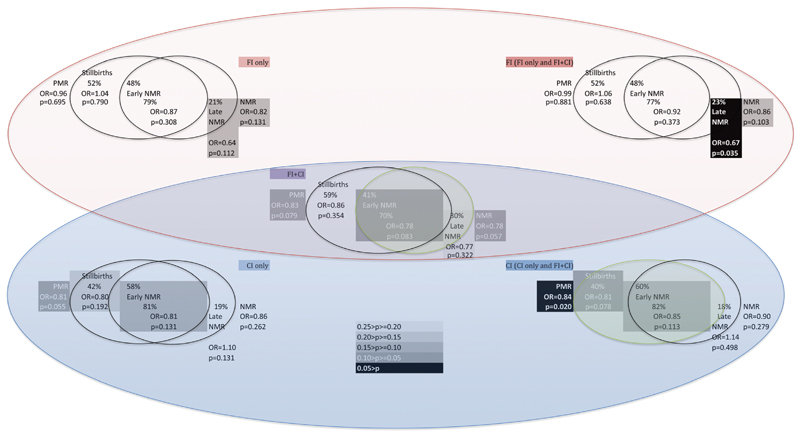
Results: For control, FI, CI and FI + CI clusters neonatal mortality rates were 34.0, 28.3, 29.9 and 27.0 neonatal deaths per 1000 live births and perinatal mortality rates were 56.2, 55.1, 48.0 and 48.4 per 1000 births, during the intervention period. Adjusting for clustering and stratification, the neonatal mortality rate was 22% lower in FI + CI than control clusters (OR = 0.78, 95% CI 0.60-1.01), and the perinatal mortality rate was 16% lower in CI clusters (OR = 0.84, 95% CI 0.72-0.97). We did not observe any intervention effects on maternal mortality.
Conclusions: Despite implementation problems, a combined community and facility approach using participatory women's groups and quality improvement at health centres reduced newborn mortality in rural Malawi.
Keywords: Malawi; Maternal mortality; Neonatal mortality; Perinatal mortality; Quality improvement; Women's groups.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- National Statistical Office (NSO), ORC Macro. Malawi Demographic and Health Survey 2004. Zomba, Malawi and Calverton, MD: NSO and ORC Macro; 2005.
-
- National Statistical Office (NSO), ICF Macro. Malawi Demographic and Health Survey 2010. Zomba, Malawi and Calverton, MD: NSO and ICF Macro; 2011.
-
- Bhutta ZA, Chopra M, Axelson H, et al. Countdown to 2015 decade report (2000–2010): taking stock of maternal, newborn, and child survival. Lancet. 2010;375:2032–44. - PubMed
-
- Zimba E, Kinney MV, Kachale F, et al. Newborn survival in Malawi: a decade of change and future implications. Health Policy Plan. 2012;27(Suppl 3):iii88–103. - PubMed
-
- Republic of Malawi Ministry of Health. Malawi 2010 EmONC Needs Assessment Final Report. Lilongwe: Ministry of Health, Malawi, UNFPA, UNICEF, WHO, AMDD; 2010.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
