

Towards elimination of the dark-rim artifact in first-pass myocardial perfusion MRI: removing Gibbs ringing effects using optimized radial imaging
- PMID: 24030840
- PMCID: PMC4176898
- DOI: 10.1002/mrm.24913
Towards elimination of the dark-rim artifact in first-pass myocardial perfusion MRI: removing Gibbs ringing effects using optimized radial imaging
Abstract
Purpose: Subendocardial dark-rim artifacts (DRAs) remain a major concern in first-pass perfusion (FPP) myocardial MRI and may lower the diagnostic accuracy for detection of ischemia. A major source of DRAs is the "Gibbs ringing" effect. We propose an optimized radial acquisition strategy aimed at eliminating ringing-induced DRAs in FPP.
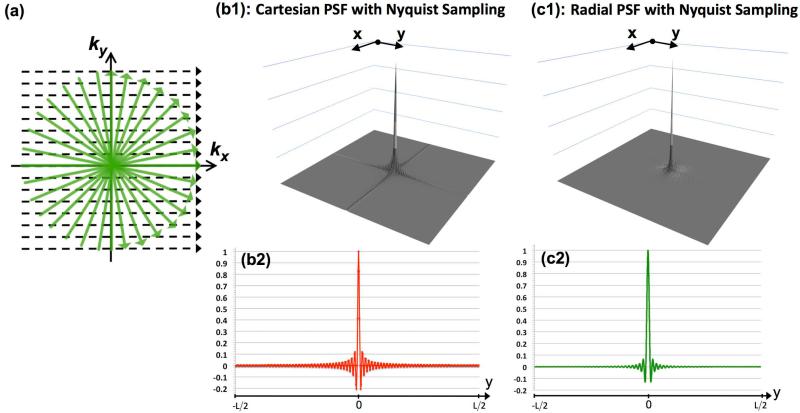
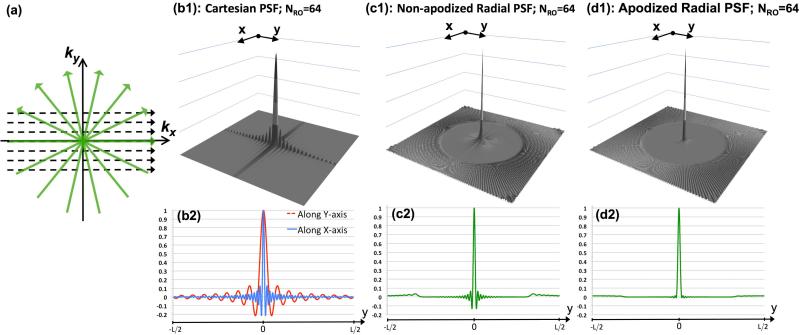
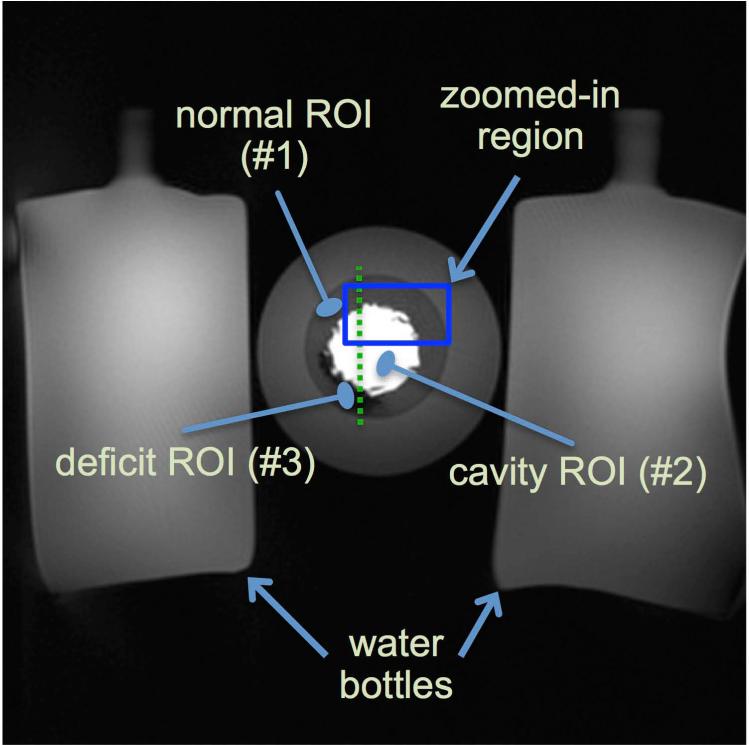
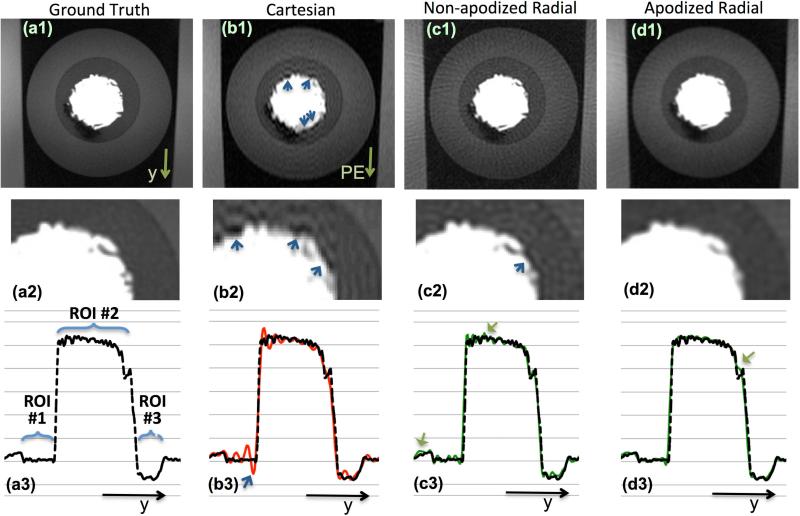
Theory and methods: By studying the underlying point spread function (PSF), we show that optimized radial sampling with a simple reconstruction method can eliminate the oscillations in the PSF that cause ringing artifacts. We conducted realistic MRI phantom experiments and in vivo studies (n = 12 healthy humans) to evaluate the artifact behavior of the proposed imaging scheme in comparison to a conventional Cartesian imaging protocol.
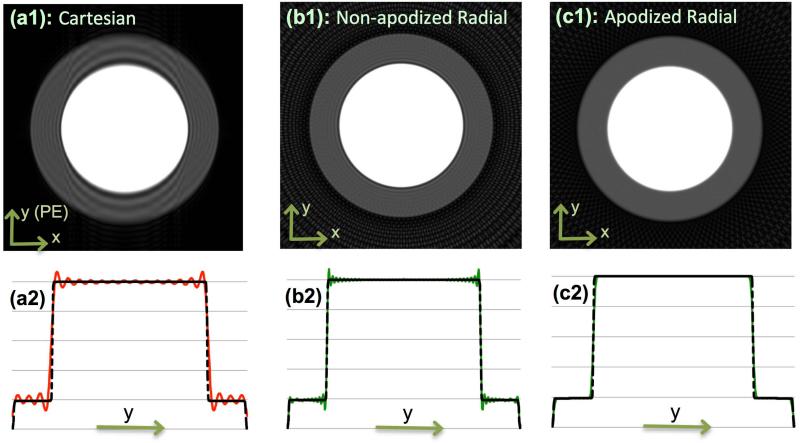
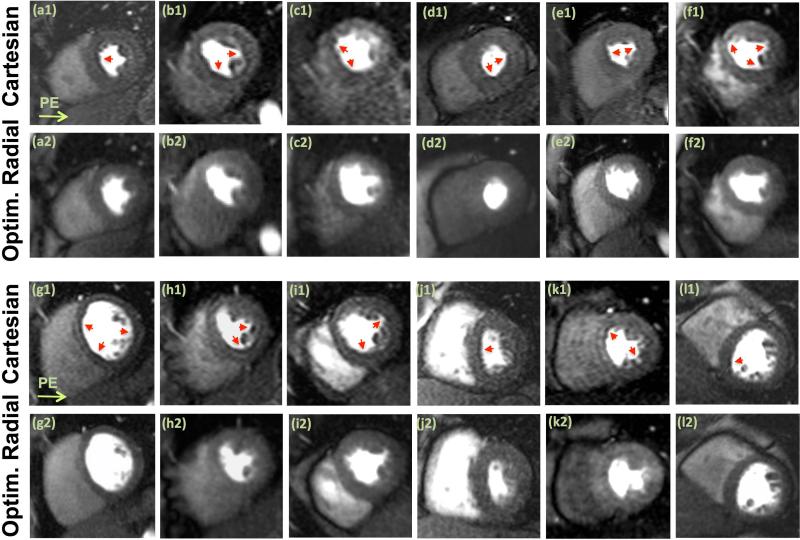
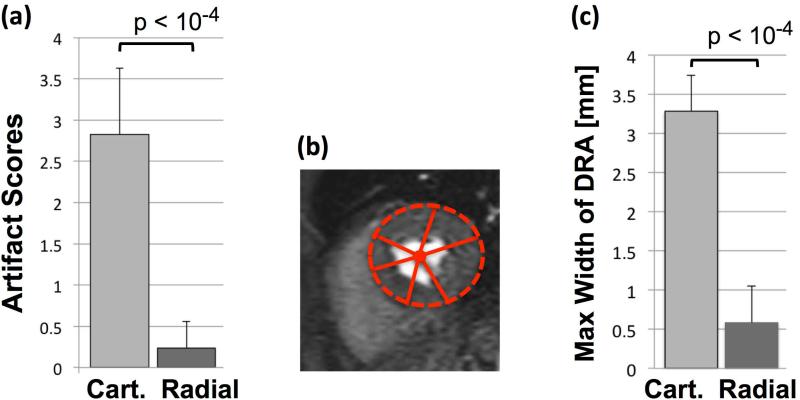
Results: Simulations and phantom experiments verified our theoretical expectations. The in vivo studies showed that optimized radial imaging is capable of significantly reducing DRAs in the early myocardial enhancement phase (during which the ringing effect is most prominent and may obscure perfusion defects) while providing similar resolution and image quality compared with conventional Cartesian imaging.
Conclusion: The developed technical framework and results demonstrate that, in comparison to conventional Cartesian techniques, optimized radial imaging with the proposed optimizations significantly reduces the prevalence and spatial extent of DRAs in FPP imaging.
Keywords: Gibbs ringing; dark-rim artifact; first-pass perfusion MRI; myocardial perfusion; radial sampling; subendocardial ischemia.
Copyright © 2013 Wiley Periodicals, Inc.
Figures
References
-
- Nesto RW, Kowalchuk GJ. The ischemic cascade: temporal sequence of hemodynamic, electrocardiographic and symptomatic expressions of ischemia. The American Journal of Cardiology. 1987;59:23C–30C. - PubMed
-
- Atkinson DJ, Burstein D, Edelman RR. First-pass cardiac perfusion: evaluation with ultrafast MR imaging. Radiology. 1990;174:757–762. - PubMed
-
- Wilke NM, Jerosch-Herold M, Zenovich A, Stillman AE. Magnetic resonance first-pass myocardial perfusion imaging: clinical validation and future applications. J. Magn. Reson. Imaging. 1999;10:676–685. - PubMed
-
- Arai AE. Magnetic resonance first-pass myocardial perfusion imaging. Top Magn Reson Imaging. 2000;11:383–398. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
